Translate this page into:
Refresher altitude chamber training for aircrew : A questionnaire feedback survey
Abstract
This questionnaire survey was conducted to get feedback from trainee aircrew about the training efficacy and operational significance of the refresher altitude chamber training. A questionnaire, consisting of 6 subsections of qualitative and quantitative questions, was designed and dispatched to 142 aircrew who had completed the refresher altitude chamber training capsule at No 1 AMTC between Jan 2002 – Dec 2003. The questionnaires were sent 2 to 6 months after completion of the training capsule. Returned completed questionnaires were divided into aircrew of the three streams and analyzed qualitatively and statistically. 74 completed questionnaires were received back (return rate = 52.1%). 77% and 72.6% of aircrew did not develop any symptoms in the hypoxia demonstration and ear clearance demonstration respectively. Commonest symptom that was reported during hypoxia demonstration was hyperventilation followed by difficulty in mental concentration. Majority of aircrew (92.8%) indicated their preference to have hypoxia demonstration at 25,000* ft or lesser altitude. Aircrew reported significant addition (average 24.1%) to their knowledge about barotrauma after the chamber training. Aircrew appreciated the physical, physiological and operational aspects of rapid decompression during the training demonstration. The average overall usefulness of altitude chamber training was 7.6 on a scale of 1 to 10. 73% aircrew reported that the training helped them in planning high altitude sorties. Pulse oximetry as a training tool was well appreciated. The feedback on altitude chamber training from the aircrew brings out that further fine-tuning, primarily in the areas of stream-specific / aircraft- specific realism and operational relevance is needed. Hypoxia demonstration needs to be improved by reviewing the simulated altitude of demonstration and by using sophisticated non-symptom based techniques to appreciate the subtle effects of hypoxia. (* one feet = 0.3048 m).
Keywords
Altitude chamber training
operational customisation
aircrew feedback

The scope of altitude chamber training, a well-established way of aircrew indoctrination in high altitude physiology, is to aid early recognition of symptoms / signs of subtle effects of hypoxia, to teach the correct use of oxygen mask and regulator, to teach and practice the Valsalva manoeuvre for clearing ears, to demonstrate effects of rapid decompression and to teach pressure breathing techniques under controlled conditions. In addition, such training helps in identification of Eustachian tube dysfunction, teaches communication while wearing a mask, especially after any oro-facial disability and identifies claustrophobia-prone individuals [1,2]. Altitude chamber training has several advantages to the aircrew and in recent literature it has been re-emphasised that these advantages are maximised when the training simulates the operational conditions physiologically [3,4].
The Ear Clearance Test (ECT), Hypoxia Demonstration (HypDemo) and Rapid Decompression simulation (RDC) protocols and the demonstration techniques used in the chamber training are time tested and have evolved over the past 30 years of training experience in the Indian Air Force (IAF). The protocols followed presently are shown in Figures 1(a), (b) and (c) respectively [5].
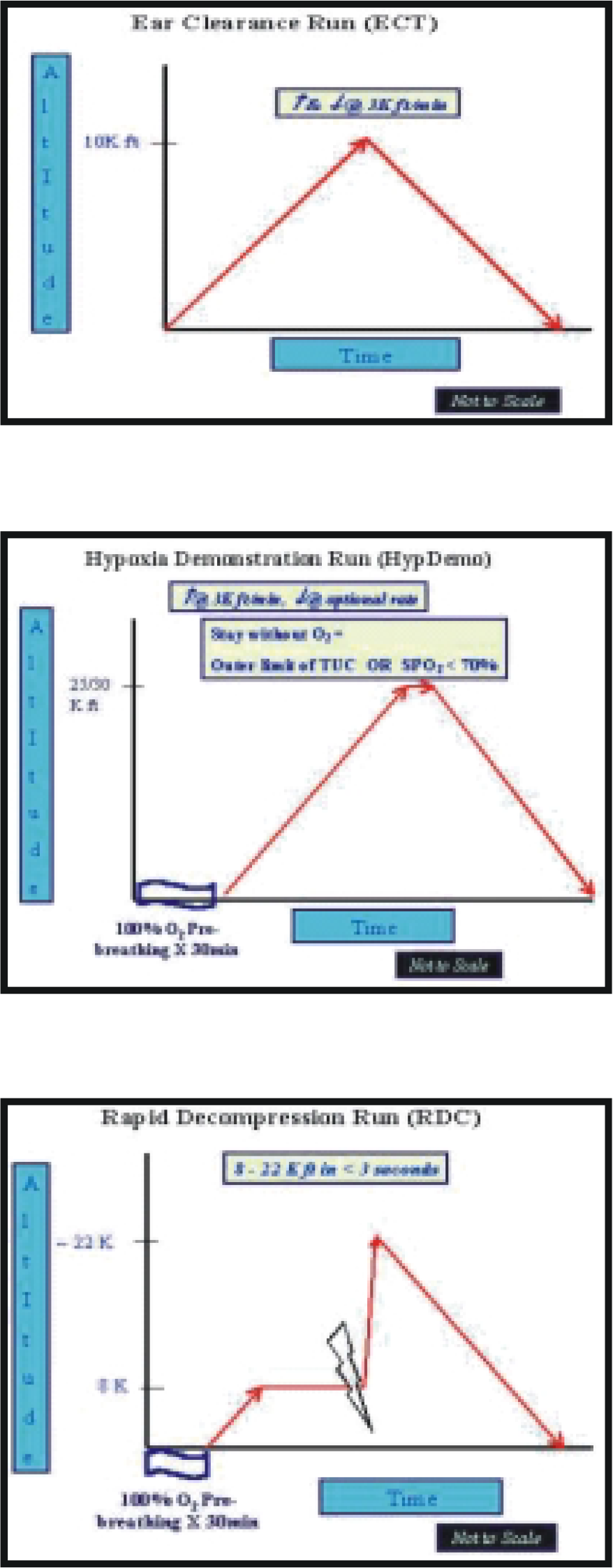
- (a), (b) & (c) : Chamber Training Protocols
Operational tactics and the flying environment have evolved over the decades in accordance with the needs of modern air warfare. Following examples, brought out by trainee aircrew during informal discussions indicated the need to review chamber training methods to match operational realism:-
Ultra-high altitude reconnaissance flying has considerably reduced as compared to the earlier decades
High altitude helicopter and unpressurised transport aircraft operations in the IAF have increased substantially [6]
Fighters are also operating from high altitude bases
No 1 Aero Medical Training Centre (1 AMTC) is primarily carrying out refresher chamber training for operationally active aircrew. It was decided to get a structured feedback from aircrew in the form of questionnaire survey as part of a larger, holistic self-audit for refresher chamber training. The approach to this audit was based on an input-output-feedback analysis model that was conceived in-house and is depicted diagrammatically in Figure 2. This self-audit also aimed to re-examine the side effects and demonstration profiles of altitude chamber training in light of the doubts cast over its side-effects visà-vis benefits recently [7,8].
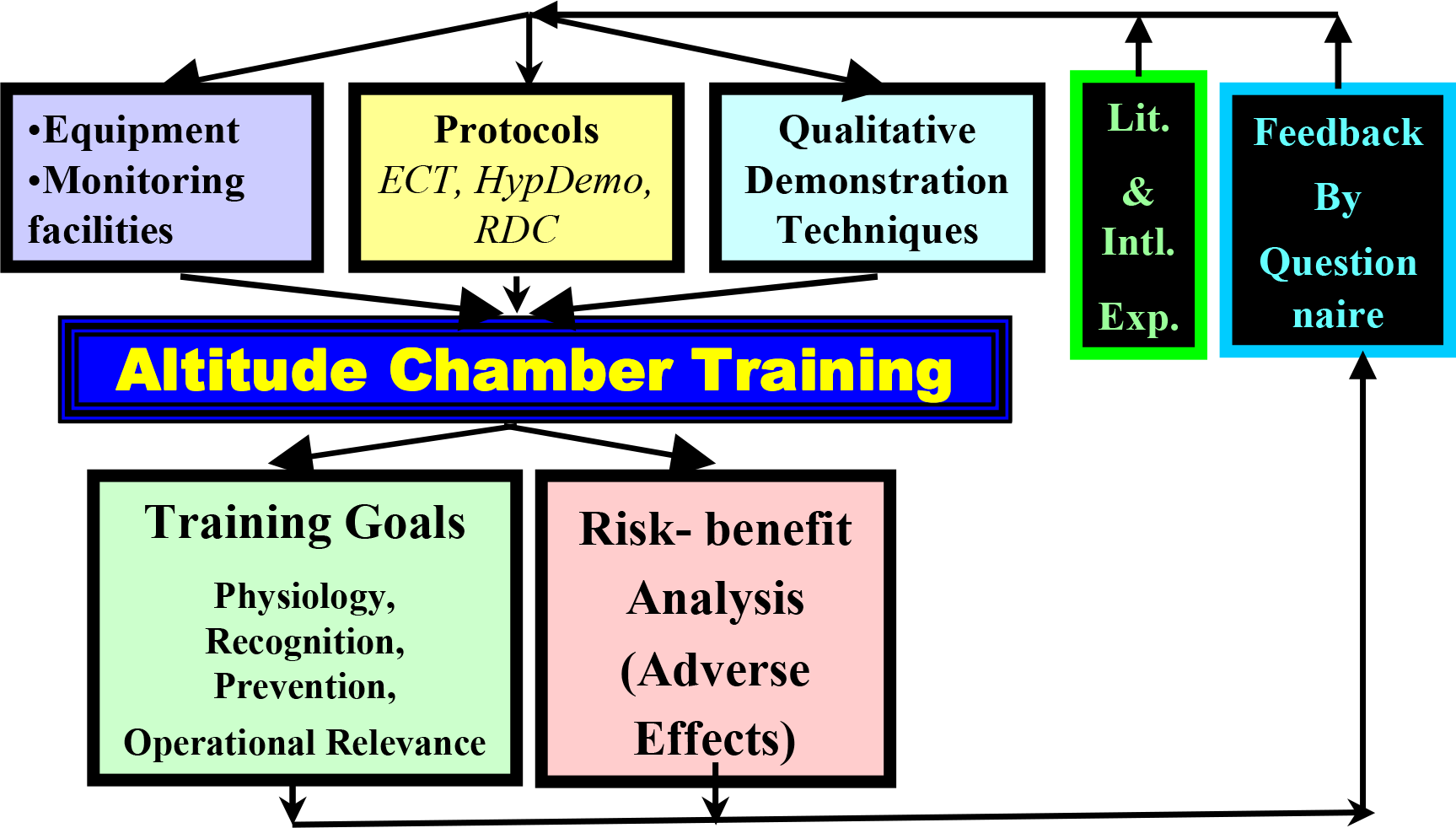
- Schematic representation of our approach
Material and Methods
A questionnaire was prepared and administered as a pilot study on five trainee aircrew. The final questionnaire, incorporating their valid suggestions, was vetted through the examiners of the Aircrew Examining Board (AEB). The final questionnaire administered to the trainee aircrew is attached as Appendix to the paper. The questionnaire comprised of a total of 30 questions that were categorized into 6 subparts viz. general particulars and flying experience, hypoxia demonstration run, ear clearance run, rapid decompression run and other information (flying clothing training, pre-run briefings and aid to sortie planning). The questionnaires were dispatched to the trainee aircrew in their units, 2–6 months after completion of the refresher chamber training and responses were sought remotely. The completed questionnaires were received back and the data segregated for the three streams of aircrew. Data was then analyzed for descriptive statistics. Unpaired ‘t’ test was applied to ascertain the statistical differences in the responses between aircrew of the three streams. A p value of 0.05 was used to determine statistical significance.
Results
Stream-wise data (fighter, helicopter and transport aircrew) of the number of respondents (with questionnaire return rates), mean age of the respondents, their total flying experience and the flying experience above 10,000 ft are summarized at Table 1. The table also shows the quantum of flying done in the period between completion of the chamber training to filling up of the questionnaire.
| Fighter | Helicopter | Transport | All | |||||
|---|---|---|---|---|---|---|---|---|
| 1. Total aircrew trained and sent questionnaire | 60 | 58 | 24 | 142 | ||||
| 2. Number of Respondents | 32 | 30 | 12 | 74 | ||||
| 3. Return rate (in %) | 53.3 | 51.7 | 50.0 | 52.1 | ||||
| 4. Mean Age (in years) | 26.1 ± 3.6 | 28.7 ± 5.2 | 27.7 ± 4.4 | 27.5 ± 4.5 | ||||
| 5. Total flying experience (in hours) experience (in hours) | 627.0 ± 527.0 | 1218.9 ± 897.1 | 1805.1 ± 1315.5 | 1037.3 ± 917.7 | ||||
| 6. Number of sorties above 10,000 ft till training | 684 ± 635.8 | 143.7 ± 157.9 | 405.0 ± 337.5 | 429.2 ± 520.4 | ||||
| 7. Period between completion of chamber training to filling up of questionnaire | ||||||||
| • Total hours flown | 57.7 ±56.2 | 136.3 ±155.7 | 487.5 ±901.4 | 101.3 ±99.4 | ||||
| • Number of sorties flown above 10,000 ft | 66.8 ±51.1 | 20.4 ±27.4 | 67.8 ±78.7 | 37.0 ±31.3 | ||||
The following inter-stream differences were found to be statistically significant:-
Flying experience before training: fighter / helicopters
Number of sorties above 10,000 ft before training: fighters/helicopters
Number of sorties above 10,000 ft after training: fighters / helicopters and fighters / transports
The following observed inter-stream differences were found to be statistically not significant:-
Age at training for all streams
Flying experience prior to training: fighters / transports and helicopters / transports
Number of sorties above 10,000 ft prior to training: fighters / transports and helicopters / transports
Total hours flown after training: between all streams
Number of sorties above 10,000 ft after training: helicopters / transports
HypDemo
Table 2 shows the data of the perception of all streams of aircrew on the following qualitative aspects of this demonstration:-
| Fighter | Helicopter | Transport | All | |
|---|---|---|---|---|
| 1. Development of symptoms during demonstration | ||||
| • Yes | 12.5 | 16.1 | 33.3 | 17.6 |
| • No | 84.4 | 83.9 | 50.0 | 77.0 |
| • No response / demonstration not done | 3.1 | 0 | 16.7 | 5.4 |
| 2. Most educative aspect | ||||
| • Recognition | 39.2 | 41.3 | 50 | 39.3 |
| • Prevention | 31.4 | 21.7 | 28.6 | 25.6 |
| • Use of mask / regulator | 17.6 | 23.9 | 21.4 | 21.4 |
| • Physiology | 11.8 | 13 | 0 | 13.7 |
| 3. Preferred hypoxia training method | ||||
| • Chamber training | 82.4 | 88.3 | 58.3 | 81.3 |
| • Lectures only | 2.9 | 5.8 | 8.3 | 5.0 |
| • Using breathing gas mixtures | 2.9 | 2.9 | 2.5 | 2.5 |
| • In air as part of flying training | 11.8 | 2.9 | 33 | 11.3 |
| 4. Usefulness of the hypoxia demonstration run | ||||
| • Highly useful | 56.7 | 43.3 | 18.2 | 45.1 |
| • Useful | 43.3 | 56.7 | 81.8 | 54.9 |
| • Useless | 0 | 0 | 0 | 0 |
Whether the aircrew appreciated any symptoms related to hypoxia
Most educative aspect of this demonstration
Preferred training method for demonstration of hypoxia
The degree of usefulness of the demonstration vis-à-vis actual operational scenarios
17.6% of the respondent aircrew appreciated symptoms of hypoxia. Various symptoms experienced are shown in Figure 3. The commonest symptom was increased rate and depth of breathing.
On a scale of 1 to 10, pulse oximetry as a tool of hypoxia understanding was rated at 7.3 by all the aircrew (fighters – 7.4, transports – 6.6 and helicopters 7.8). The differences in responses between the helicopter and transport crew were found to be statistically significant.
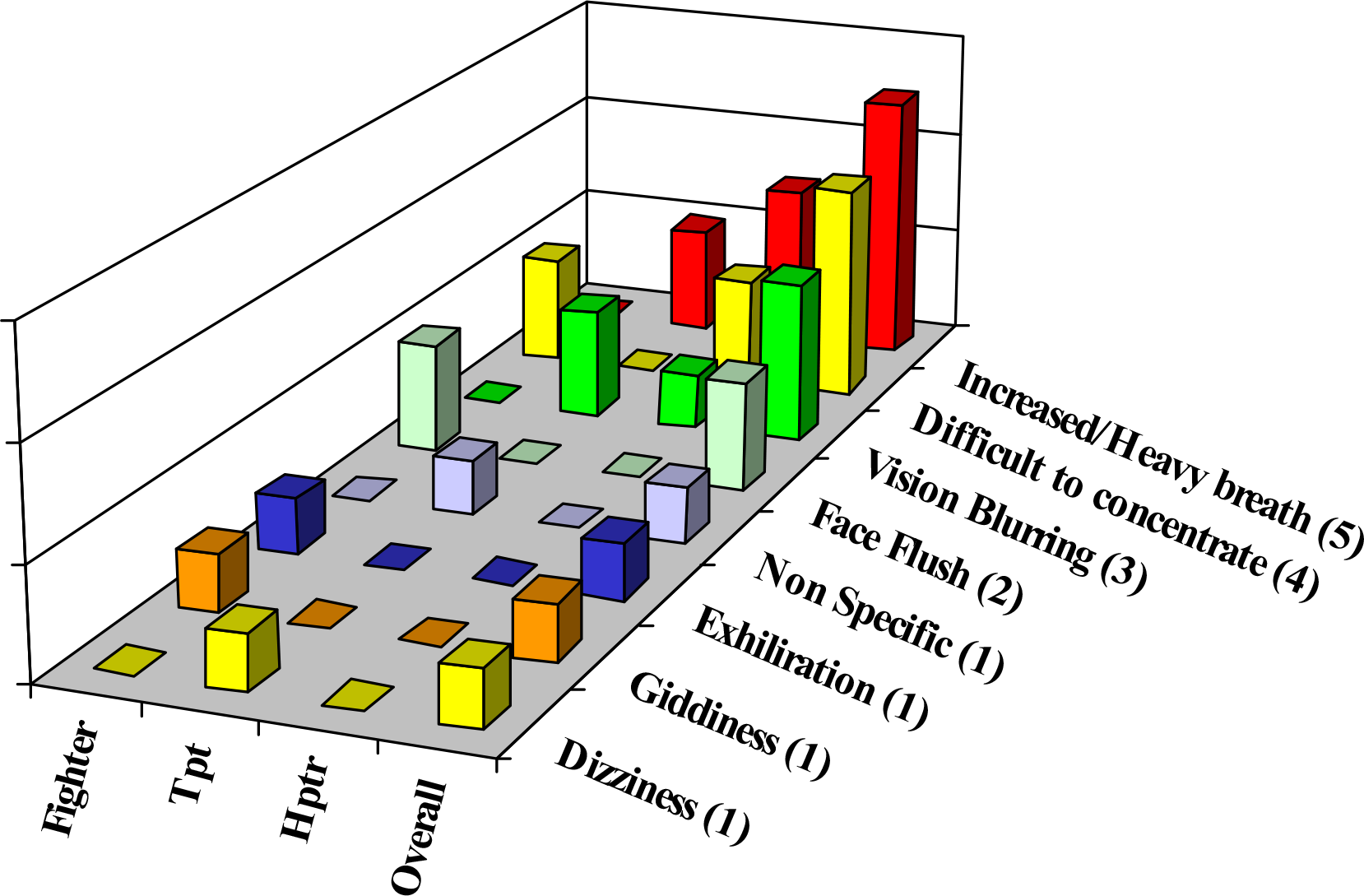
- Symptoms during hypoxia demonstration
- (Figures in Brackets = Number of Respondents)
Figure 4 shows the simulated chamber altitude at which aircrew of various streams would prefer their hypoxia training to be carried out to match their operational needs. Overall, most preferred and operationally relevant training altitude reported was 18,000 to 25,000 ft (49.3% of all respondents). Only 2.9% of the respondents (all fighter pilots comprising of 6.6% of the total fighter aircrew respondents) preferred the presently prescribed altitude of 30,000 ft. 29% and 36.4% of the fighter pilots also preferred training to be carried out at < 18,000 ft and between 18,000 – 25,000 ft altitude respectively. 100% of the helicopter aircrew expressed that their training should be carried out below 25,000 ft and 75% of transport aircrew respondents felt 18,000 – 25,000 ft is the operationally most suited altitude to demonstrate hypoxia to them.
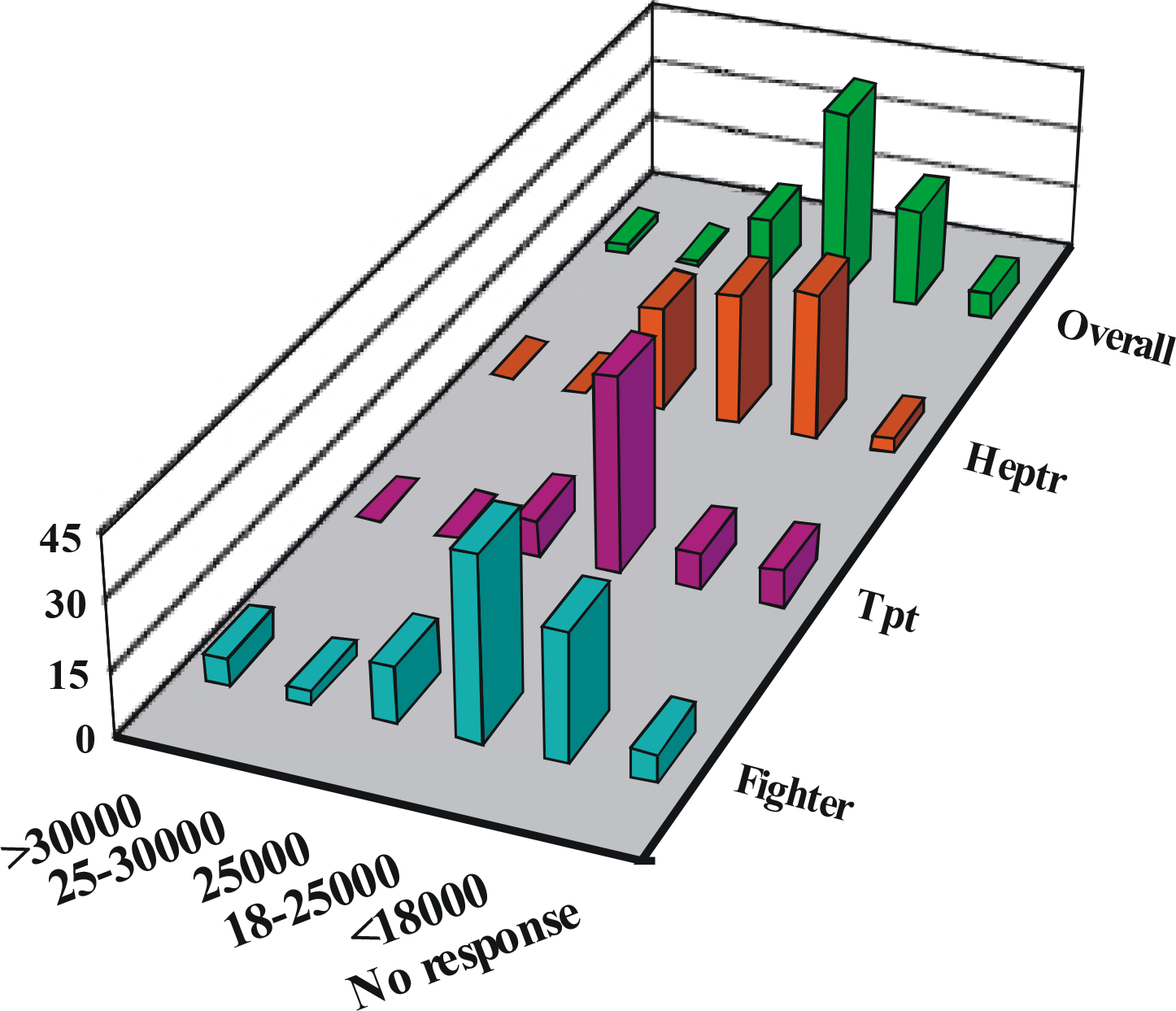
- Hypoxia Demonstration - Most preferred altitude
ECT
Table 3 shows the stream-wise feedback on the ECT demonstration run:-
| Fighter | Helicopter | Transport | All | |
|---|---|---|---|---|
| 1. Experienced barotrauma symptoms | 19.4 | 30.0 | 41.7 | 27.4 |
| 2. Most educative aspect of the demonstration | ||||
| • Valsalva manoeuver | 33.3 | 47.2 | 30 | 38.5 |
| • Causes | 30.9 | 16.7 | 30 | 25.0 |
| • Prevention | 33.3 | 36.1 | 40 | 35.4 |
| • Others | 2.4 | 0 | 0 | 1.1 |
| 3. Level of barotrauma related awareness before and after the training * | ||||
| • Before training | 64.1 ±18.5 | 64.3 ±17.2 | 50.8 ±17.8 | 62.0 ±18. |
| • After training | 85.8 ±9.2 | 88.7 ±11.8 | 80.4 ±12.1 | 86.1±11.1 |
| • Improvement | 21.7 | 24.4 | 29.6 | 24.1 |
| 4. Operational usefulness of the training | ||||
| • Highly useful | 41.9 | 56.7 | 47.9 | 47.9 |
| • Useful | 58.1 | 43.3 | 52.1 | 52.1 |
| • Useless | 0 | 0 | 0 | 0 |
Ability to demonstrate barotrauma related symptoms
Most educative aspect of the ear clearance run
Levels of barotrauma related awareness before and after the training
Operational usefulness of this training
RDC
The stream wise distribution of the ability of this run to demonstrate the physical effects (noise, drop in temperature, misting) and physiological effects (respiratory symptoms) of rapid decompression are shown in Table 4. The table also shows the operational usefulness of this run as perceived by the aircrew.
| Fighter | Helicopter | Transport | All | |
|---|---|---|---|---|
| 1. Ability to demonstrate physical effects (scale of 1 – 10) * | 7.8 ±1.1 | 7.7 ±1.3 | 8.2 ±1.3 | 7.8 ±1.2 |
| 2.Ability to demonstrate physiological effects (All figures in %) | ||||
| • Yes | 90.6 | 66.7 | 75.0 | 78.4 |
| • No | 0 | 0 | 0 | 0 |
| • Somewhat | 9.4 | 23.3 | 25.0 | 17.6 |
| • No response | 0 | 10 | 0 | 4.0 |
| 3. Operational usefulness of the training run (scale of 1 – 10) * | 7.2 ±1.3 | 6.6 ±2.2 | 7.3 ±1.1 | 7.0 ±1.6 |
* inter-stream differences statistically not significant
Other aspects of refresher chamber training
Table 5 summarizes the responses of aircrew in respect of the adequacy of protective flying clothing related training, overall usefulness of this training for their flying careers and the practical application of the knowledge gained by them in planning sorties above 10,000 ft. All the aircrew who underwent training were satisfied with the depth and scope of the pre and post demonstration briefings.
| Fighter | Helicopter | Transport | All | |
|---|---|---|---|---|
| 1. Protective flying clothing demo usefulness (in %) | ||||
| • Useful | 78.8 | 90 | 100 | 87.7 |
| • Not useful / no gain in knowledge | 21.2 | 10 | 0 | 12.3 |
| 2. Composite usefulness of refresher chamber training in flying career (scale of 1 – 10) * | 7.8 ± 1.3 | 7.3 ± 1.8 | 8.1 ± 1.1 | 7.6 ± 1.5 |
| 3. Post-training usefulness of the training in planning sorties above 10000 ft (in %) | ||||
| • Useful | 74.9 | 73.3 | 58.3 | 73.0 |
| • Not useful | 22.0 | 16.7 | 16.7 | 17.6 |
| • Did not fly above 10,000 ft since the training | 3.1 | 10 | 25 | 9.4 |
* inter-stream differences statistically not significant
Discussion
Hypoxia has once again come under the focus of operational safety world over in the 1990’s after the highly-reported hypoxia-induced fatal aircraft accident that occurred in an unpressurised fixed-wing aircraft with altitude ceiling of 10,000 ft [9]. An analysis of military helicopter accidents in high altitude areas in India brought out that hypoxia may have been at least partly responsible for a number of mishaps [10]. In the Indian context, increased military operations and adventure activities in the high altitude terrain have brought out the vulnerability of the aircrew to its side effects [11]. It can be said that hypoxia today is a greater problem in unpressurised aircraft (including helicopters) flying at the extremes of physiological compensatory limits, than in ultra-high flying aircraft that have dependable life support systems. Similar reported mishaps have re-emphasised the importance and operational focus of high altitude training for aircrew [2,5].
Feedback from trainee aircrew on altitude chamber training, an input with operational ramifications, has not been reported in the Indian aeromedical literature for a long time. This is possibly because the training profiles and the demonstration techniques had been fine-tuned since the 1960’s through the 1980’s. This study has attempted to address this important facet of operational relevance of refresher altitude chamber training by ascertaining the views of the operational aircrew.
Questionnaire survey as a research methodology
A questionnaire survey is a useful research tool with the potential of ascertaining the views of respondents on specified issues [12]. The questionnaires need to be correctly worded since leading questions could vitiate the true findings. Questionnaire analysis also has limitations of interpretations and should be viewed as a research tool with limited diagnostic sensitivity and specificity. However, the responses to the questionnaire surveys do indicate subjective trends effectively. Hence the construction of the questionnaire and the interpretation of the results of this survey should be viewed in the light of these limitations.
The questionnaire used in this study was developed locally and tested in a pilot study on five trainee officers and aircrew examiners at the AEB. Despite these attempts, certain avenues still exist for further refinement of our questionnaire.
The questionnaires were administered remotely after a delay of few weeks and were not given immediately during or on immediate completion of the refresher-training capsule. This was done for the following reasons:-
To allow time for the actual practical application of the knowledge imparted during training by the aircrew in their respective operational flying conditions before responding to the questionnaire.
To avoid colouring of responses by the desire to do well in the examination at the end of the refresher training capsule.
General details of the participants
In our general data of respondents, there is a large variation in the flying experience and number of sorties flown above 10,000 ft. This is because of basic differences in the flying task and missions flown by aircrew from the three streams (fighters, helicopters and transport). However, within a given stream also, the variations are large. This is mainly because the Indian topography is varied and the IAF has a large inventory of aircraft, which exposes the aircrew during their flying careers to varied types of flying, including high altitude flying. Another important reason for this variability is that aircrew of varying ages and flying experiences attend the refresher chamber-training capsules, unlike in some countries where the aircrew undergo hypoxia training at fixed periodicity (e.g. every 3/5 years) [13,14]. In the IAF, no such specified periodicity is being practically followed. In this regard, we also agree with the suggestions given by some aircrew to conduct special targeted refresher chamber training, as and when a particular aircrew is posted / re-posted to units flying aircraft at high altitudes / operating from the high altitude areas.
HypDemo
Our data suggests that refresher hypoxia demonstration, as carried out in our centre, is well appreciated by the aircrew. The training has been practical oriented and focused more on its practical usage by the aircrew in flight than on theoretical aspects. This approach, with its operational benefits, is recommended [2,5].
Large number of aircrew did not experience any symptoms of hypoxia during the demonstration. In these trainees, the ‘hypoxia recognition’ was solely dependent on objectively demonstrating the deterioration of mental and visual functions during the run. We used simple arithmetic calculation sheets and handwriting deterioration demonstration for this purpose. We also developed a worksheet based on the actual in-flight calculations that aircrew need to do in conjunction with the AEB (this, to be solved by the aircrew on ground and in-chamber to assess their own accuracy and speed of calculations). Further, stream and aircraft specific refinements to this worksheet are envisaged to make it more customised to individual trainee’s needs. We demonstrated night vision deterioration using aviation maps and color discs at 18,000 ft during the ‘descent’ phase of the demonstration.
To emphasize the importance of combating hypoxia and to make the demonstration more educative we also used pulse oximetry (SPO2) monitoring in the following ways:-
To show the rapidity with which SPO2 falls below 90% at demonstration altitude
To show the changes with hyperventilation and muscular exercise (repeated voluntary arm muscle tensing)
To re-emphasise the correct use of regulators and mask (effect of wearing a loose mask, disconnection from regulator)
The overall satisfaction for pulse oximetry as a training tool was high (7.4 on a scale of 1 -10) and this tool must be made use of in training. The helicopter pilots appreciated this technique most, mainly because of their greater awareness of the technique that was used in the development of helicopter oxygen systems in the recent past. In addition to being a training tool, pulse oximetry based SPO2 monitoring is a good indicator to terminate the run (SPO2 < 70%).
A variety of more sophisticated computerized techniques that can more objectively demonstrate the subtle cognitive effects of hypoxia are available and well validated. These include Flight Orientation Performance Task (FOPT), Automated Psychomotor Assessment System (APAS) etc. [15,16,17]. A detailed comparative analysis of all these methods is considered beyond the scope of this paper but based on our data we strongly feel that these techniques need to be routinely used in all our hypoxia training.
81.4% aircrew consider chamber training as the ideal method of hypoxia training. Only 2.5% aircrew reported that they would prefer gas mixtures based hypoxia simulation training, clearly indicating its operational irrelevance to them. 11.3% of the respondents, consisting of transport and fighter pilots, feel that more frequently practiced hypoxia related emergencies in-flight (e.g. practice emergency – pressurization failure) would be most beneficial in their hypoxia training. This point has merit and needs further consideration by the respective flying training establishments and flying supervisors.
Our study shows that majority of aircrew (92.8%) would prefer refresher chamber training at or below 25,000 ft simulated altitude. At present the training is recommended to be carried out at 30,000 ft and only 2.2% aircrew prefer that altitude for training. There are thus differences in the prescribed training altitude and the actual operational needs of the aircrew. For example, training altitude of 30,000 ft may be envisaged to be too high for helicopter aircrew who rarely fly above 18,000 ft and almost never above 21,000 ft. On the contrary, in the IAF context, it can be argued that training at 30,000 ft will benefit them subsequently if and when they fly pressurized fixed wing trainer aircraft (when some of them become flying instructors).
Some of the international centers are following an altitude of 25,000 ft as hypoxia demonstration altitude, especially for refresher chamber training [14,18]. An important consideration for training at lower altitudes is the reported greater incidence of Decompression Sickness (DCS) at higher altitudes. In our recent 6-year database of chamber-related side effects in the IAF we did not find any incidence of DCS and hence have no evidence to recommend lower demonstration / training altitudes for preventing DCS [5]. Training at lower altitudes allows greater time for the trainee to understand the subtle effects of hypoxia more comprehensively since the effects set in slowly. Due to this, the operational needs of the aircrew and the possibility of higher incidence of DCS at higher altitudes, we also strongly feel that for refresher hypoxia-training (vis-à-vis ab-initio chamber training) training altitudes must be reduced from the presently recommended 30,000 ft to that based on stream of aircraft flown. We also feel that for refresher training, there is a case for customising the training altitudes to the specific operational needs of the trainees rather than following a fixed prescribed training altitude.
ECT. This demonstration run acts as both an ear patency check prior to other demonstration runs and as a Valsalva manoeuver practice session. Responses of the aircrew indicate that the theory, causes and preventive aspects of barotrauma were well appreciated by them. The training has benefited the aircrew (subjective average improvement of 24.1%).
RCT. This run is able to demonstrate the physical and physiological effects of sudden loss of pressure and aircrew appreciated the operational usefulness of the run. Interestingly, aircrew who fly unpressurised helicopters also responded to the feedback and their responses were not significantly different from those of aircrew flying fixed-wing pressurised aircraft. It is pertinent to bring out that in our experience the helicopter aircrew are reluctant to undergo this run as they consider it irrelevant to their day-to-day operational flying. This was also confirmed from our study of six-year chamber training analysis in the IAF [5]. The reasoning put forward by these aircrew in not subjecting themselves to this run, especially during refresher training (vis-à-vis ab-initio chamber training), has merit.
Other points. The feedback indicates that aircrew have largely appreciated the flying clothing related training that teaches them to test their own clothing. Some of the fighter aircrew expressed quality control related views in the answer to this question and hence their rating appears to be the least. The aircrew were satisfied with the extent and depth of briefings done prior to each run. Data suggests that 73% of aircrew actually utilized the training operationally within about 6 months of training. The overall rating of 7.6 (on a scale of 1 – 10) given to the chamber training is also highly satisfactory.
Conclusion
Our data suggests that aircrew appreciate the scope of refresher chamber training and the importance of the individual runs. The training is practical and oriented towards in-flight problem solving. There is a scope to make hypoxia training more realistic by introducing more sensitive demonstration techniques and following more realistic simulated flight protocols. This feedback has given useful inputs to improve upon refresher altitude chamber training.
References
- The Historical Perspectives In: Dehart RL, ed. Fundamentals of Aerospace Medicine. Philadelphia: Lea & Febiger; 1985. p. :14.
- [Google Scholar]
- Quick responses by pilots remains key to surviving cabin decompression. Human Factors and Aviation Medicine. 2000;47(1) Web page http://www.flightsafety.org/members/serveme.cfm?path=hf/hf_jan-feb00.pdf Accessed on 15 Mar 2003
- [Google Scholar]
- Time of useful consciousness determination in aircrew members with reference to prior altitude chamber experience and age. Aviat Space Environ Med. 2000;71:72-6.
- [Google Scholar]
- In-flight hypoxia incidents in military aircraft: Causes and implications for training. Aviat Space Environ Med. 2003;74:169-72.
- [Google Scholar]
- A retrospective analysis of altitude chamber training protocols and the adverse effects at Aero Medical Training Centers in the Indian Air Force: 1998-2003. Paper presented at 52nd International Congress on Aviation and Space Medicine 2004.
- Altitude Chamber Training: Is it worth the risk? 1992. Human Factors and Aviation Medicine. 39 Web page http://www.flightsafety.org/members/serveme.cfm?path=hf/hf_sep-oct92.pdf Accessed on 15 Mar 2003
- [Google Scholar]
- 2002. Web page http://www.defence.gov.au/news/raafnews/EDITIONS/4405/story01.htm Accessed on 15 Mar 03
- [Google Scholar]
- Pilot incapacitation by Hypoxia cited in fatal five-hour flight of Beach King Air In: Accident Prevention. Vol 59. p. :1-7.
- [Google Scholar]
- Aircraft accidents in Indian Army Aviation–A general review since its inception. Ind J Aerospace Med. 1996;40(1):7-21.
- [Google Scholar]
- Hypoxia : the silent operator in helicopter flying. Ind J Aerospace Med. 2001;45(2):76-82.
- [Google Scholar]
- Basics of Developing Questionnaires. 1999. Web page http://www.managementhelp.org/commskls/qustnair/qustnair.htm Accessed on 20 Mar 03
- [Google Scholar]
- Web page www.jsc.nasa.gov/jao/pdf/app-g.pdf Accessed on 12 Mar 03
- [Google Scholar]
- United States Army School of Aviation Medicine. Flight Physiology branch. web page http://usasam.amedd.army.mil/_Flt_Physiology/chamber.htm accessed on 17 Mar 03
- [Google Scholar]
- Ind J Aerospace Med. 1997;41(2):80-88.
- [Google Scholar]
- Altitude Chamber Experiences. Web page http://www.noaa.inel.gov/Capabilities/longEZ/pdf/hypoxia.pdf posted on 26 Feb 2002 Accessed on 16 Mar 03
- [Google Scholar]
- Environmental Tectonics Corporation. Web page http://www.etcbiomedical.com/hbo_apas.htm Accessed on 11 Mar 03
- [Google Scholar]
Appendix
Proforma for feedback on Decompression Chamber (DC) training at No.1 AMTC
Personal details
Name:
Rank:
Service No:
Unit:
Type of aircraft on which current:
Age at the time of DC training:
Hours flown after completion of DC course:
Number of sorties above 10,000 ft flown till date:
Number of sorties flown above 10,000 ft flown after DC training: -----------------------------------------------------------------------------------------------------------------------
Hypoxia indoctrination demonstration run Did you develop any symptoms during the run? Yes / No If yes, describe the symptoms briefly : ______________________________ Hypoxia demo was most educative about which aspect of Hypoxia in flight? Recognition Prevention Use of Mask / regulator Physiology of Hypoxia Pulse Oximetry was used to demonstrate the rapidity with which Hypoxia can set in. On a scale of 1 to 10, (1 = least valuable, 10 = highly valuable) indicate the value of Pulse Oximetry in Hypoxia Demo as perceived by you. ________________ In your opinion, what would be the best method of demonstrating hypoxia to the aircrew? Chamber training Lectures only Using ground-based breathing gas mixtures In air, as part of flying training The altitude chamber demonstration was given at simulated altitude of 25,000 ft. Indicate the altitude that you consider most suitable to simulate your flying environment. <18,000 ft 18,000 – 25,000 ft At 25,000 ft (as of now) >25,000 ft 30,000 ft Which aspect of Hypoxia Demo made the most impact on you? None Recognition (with Pulse Oximetry) Recovery aspects Usefulness of this training in your flying career. Highly useful Useful Useless Ear clearance run Did you develop any symptoms during this demo? Yes / No Which aspect of this demo was most educative? Valsalva training Causes of barotrauma Prevention factors Others (Pl specify) On a % scale, indicate your level of awareness about barotrauma before and after the course: Before: _____% After: ______% Usefulness of this simulated run in your flying career. Highly useful Useful Useless Rapid decompression run (In the rapid decompression run, the chamber was decompressed from simulated altitude of 8000 ft to about 22,000 ft) On a scale of 1 – 10 (1 = not effective, 10 = highly effective), indicate if the demonstration was effective in demonstrating the physical effects (noise / misting etc.) of a cabin rapid decompression? __________ Did the demonstration adequately demonstrate the effects of rapid decompression on your respiratory system? Yes No Somewhat Indicate on a scale of 1 – 10, how much would the chamber experience help you in tackling rapid decompression if it were to occur in flight. __________ Flying clothing demonstration Did you benefit from this training in terms of understanding the physiological QRs & field-testing of your flying clothing? Yes No Somewhat General feedback Were the briefing and the de-briefing procedures adequate? Yes No On a scale of 1 –10 (1 = no relevance, 10 = highly relevant), indicate your perception of the overall usefulness of the decompression chamber training in your flying career. ____________ Did the decompression chamber training help you subsequently in planning sorties above 10000 ft? Yes No Somewhat Any other topics of high altitude physiology that you feel should be covered during the training? ___________________ Any other suggestions regarding this training?




