Translate this page into:
Retrospective analysis of initial medical examination of aircrew applicants in the Indian Air Force
Abstract
Indian Air Force (IAF) ensures physical fitness of candidates before selection for aircrew duties through a stringent medical examination. The medical standards for aircrew candidates have been specified in detail and are updated regularly. Literature search did not reveal any published study in the IAF on the nature of disabilities detected during initial medical examination of aircrew candidates. This study was carried out to analyze the pattern of medical conditions resulting in disqualification among National Defence Academy (NDA) candidates. Detailed records of all medical examinations carried out at the Institute of Aerospace Medicine are maintained at Medical Evaluation Centre. These records of NDA candidates were accessed for the period 1997-2004 for analysis in this study. Out of632 candidates examined during this period, a total of 229 (36.2 %) were disqualified for aircrew duties. Some of these candidates had more than one disability. Overall, 275 disqualifying disabilities were found in these 229 candidates. Out of these, the commonest were ophthalmologic conditions (35.8%), followed by radiological spinal abnormalities (23.9%) and anthropometric incompatibility (14.4%). The proportion of applicants made unfit for aircrew duties reflects the significance of stringent, detailed and thorough medical examination at entry. AB these disabilities were detected in asymptomatic individuals. The importance of continuously evolving stringent medical standards for aircrew duties is discussed.
Keywords
Aircrew candidates
medical examination
fitness

Military aviation demands extraordinary level of physical fitness among aircrew. To fulfill this objective, stringent criteria for medical examination are laid down. This is necessary for training as well as for further employability and to minimize drop out as training costs for aircrew training are prohibitive.
Indian Air Force (IAF) ensures this objective through a comprehensive medical evaluation of candidates before they are recruited for flying training. Standards for these medical examinations are stipulated in IAP-4303 (3rd Edition). This document enlists in detail, methods of medical examination as well as criteria applicable for initial medical examination of aircrew candidates.
IAF selects pilots through National Defence Academy (NDA) and Combined Defence Services Examination (CDSE). NDA candidates are in a lower age group (16 to 22 years) as compared to CDSE candidates who are between 21-26 years of age. This age difference has been kept in mind while laying down various preselection criteria as well as certain waivers.
Literature search did not reveal any published study analyzing the medical conditions leading to unfitness for aircrew duties at entry in IAF. A study of such kind can provide useful insight regarding adequacy of existing policies related to selection criteria and prevalence of medical disabilities. The present study was therefore carried out to analyze the medical conditions causing unfitness among aircrew candidates at the Institute of Aerospace Medicine (IAM).
Material and Methods
Records of all preselection medical examinations are maintained at Medical Evaluation Centre in IAM. These records of aircrew medical examinations for the past eight years (1997-2004) were accessed and included for analysis. All candidates undergo the full sequence of medical examination as per IAP 4303 irrespective of disability being detected at any stage of examination.
Some candidates, had more than one disqualifying disability, therefore, the number of disabilities referred in the study is greater than the number of total unfit candidates. In candidates with multiple medical disabilities, only those co iditions have been considered that were cause for permanent unfitness.
Results
A total of 632 NDA aircrew candidates underwent medical evaluation during the period of study. The mean age was 17 years (range 16-22 years). A total of 229 candidates (36.2%, n=229) were made unfit for Air Force duties because of medical disabilities.
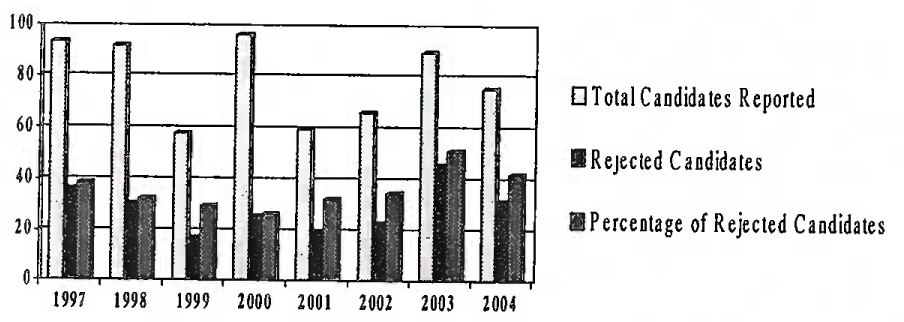
- Yearwise breakup of NDA candidates reported and rejected
Figure 1 depicts that percentage of rejected candidates is showing an increasing trend over the last 3 years.
Ophthalmologic conditions (37%), radiological spinal anomalies (24%) and anthropometric incompatibility (14%) were the three major groups causing medical unfitness in these candidates (Fig 2) and accounted for 75% of the disabilities. Otorhinolaryngological, general medical, orthopedic and surgical conditions constituted remaining 25% of the disabilities.
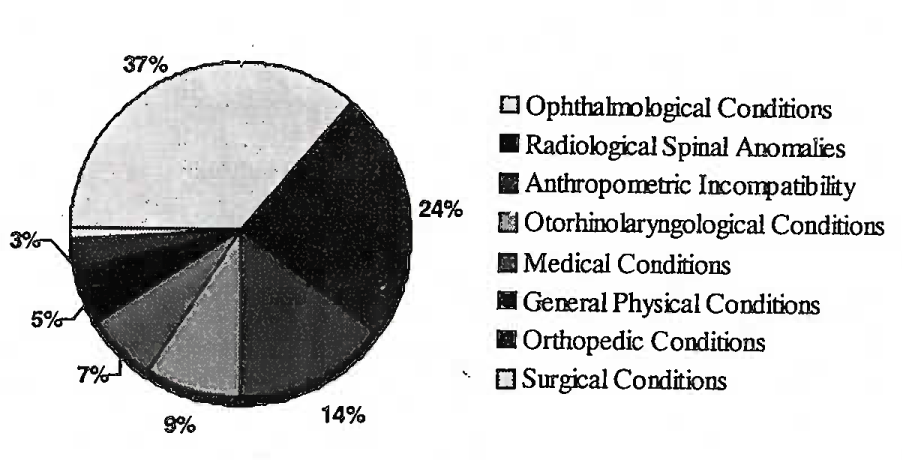
- Disqualifying conditions in candidates
Refractive error (substandard vision) constituted more than three-fourths of the disqualifying ophthalmologic conditions (76%, n=99), commonest of these being myopia (Fig 3).
Common radiological findings responsible for disqualification were lumbosacral anomalies like unilateral and bilateral complete/incomplete sacralisation/ lumbarisation (35%) and anterior wedge compression fracture of vertebral body (20%). Degenerative conditions like intervertebral disc disease (20%), spondylosis (14%) and spondylolysis (11%) were other significant radiological spinal anomalies (Fig 4).
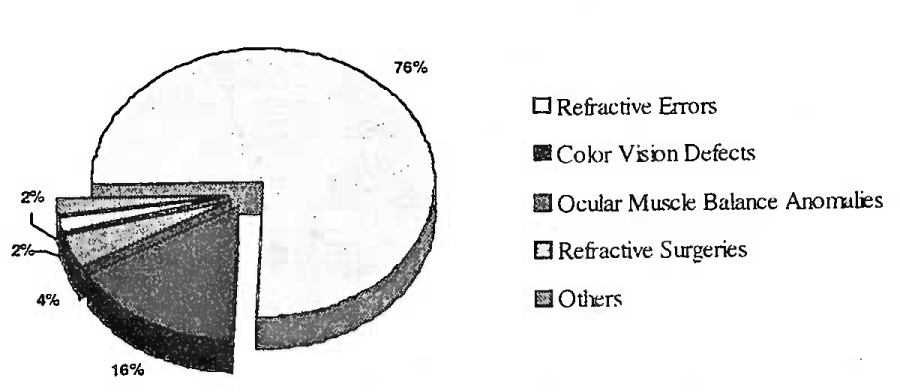
- Ophthalmological conditions
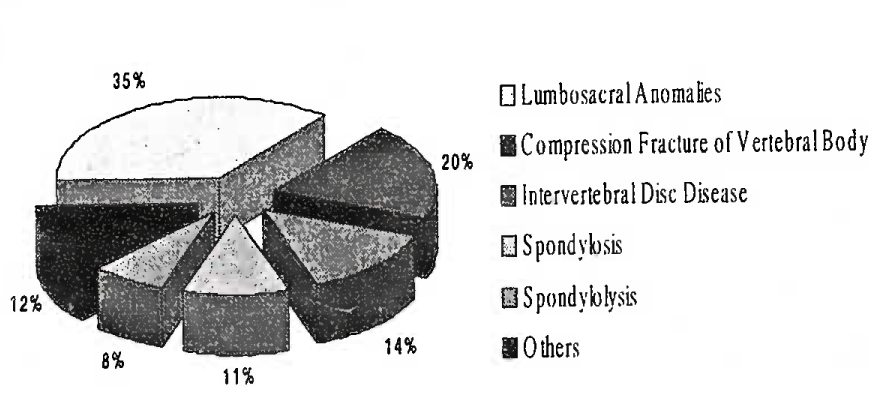
- Radiological abnormalities
Anthropometric incompatibility based on accepted IAF standards in candidates was one of the important causes of disqualification. Commonest anthropometric condition being substandard leg length measurements (27%), substandard sitting height (19%) and substandard height (15%) (Fig 5).
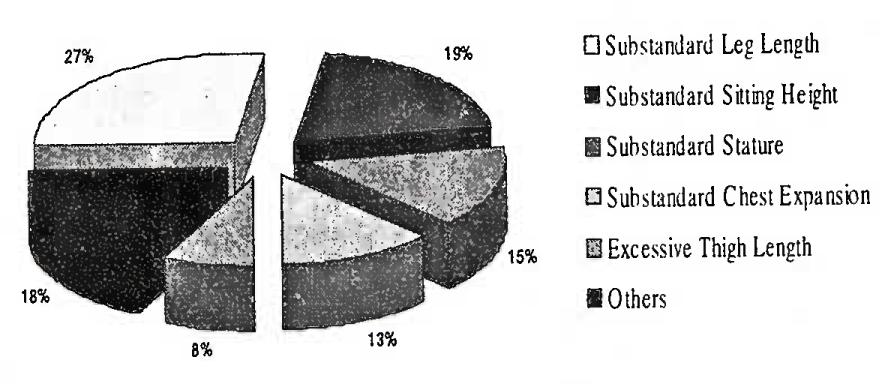
- Anthropometric incompatibilities
Otorhinolayngological conditions formed 9% of total disabilities causing unfitness. Commonest disqualifying otorhinolaryngological conditions were deviated nasal septum, audiometrie hearing loss and external ear pathologies viz congenital anomalies, persistent infection (Fig 6). Other disqualifying otorhinolaryngological conditions included middle ear disease, external ear anomalies and tonsillar hypertrophy.
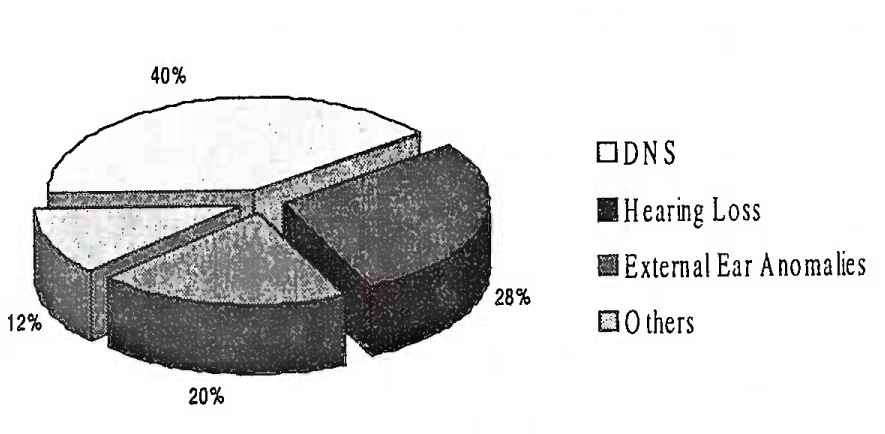
- Otorhinolaryngological conditions
Among general medical conditions, cardiovascular system anomalies viz. ECG abnormalities, cardiac murmur and hypertension formed 50% of the medical disabilities which led to rejection. About 17% of disabilities were related to central nervous system viz. EEG abnormalities. Sporadic disqualifying conditions were seen in respiratory and gastrointestinal systems.
General physical conditions were among other disqualifying conditions and contributed to 5% of all disabilities (Fig 2). Majority of these were candidates who were obese/overweight except a single case who was underweight.
Orthopedic conditions were responsible for a small percentage of disqualifying disabilities (Fig 2). Knee abnormalities viz. genu varum, genu valgum were common along with few cases of flat feet, old fracture-deformity of long bones.
Surgical disabilities were the minor contributor towards disqualifying disabilities (Fig 2). These included hydrocoele, renal calculi and congenital renal anomaly.
Discussion
During the eight years covered under this study, almost one-third of the NDA candidates were rejected on account of various medical disabilities. This is a significant percentage as almost all the candidates reporting for medical examination were asymptomatic. This corroborates well with the stringent medical evaluation system of 1AF. Similar findings have been reported by Khazaleh et al who found a rejection rate (31.3%) among candidates on medical grounds in the Royal Jordanian Air Force (RJAF) [2].
Ophthalmologic conditions
Ophthalmologic conditions were the commonest causes for disqualifying disabilities in the present study. Refractive error is the commonest cause of diminished vision in general population and this was observed among the candidates. Other workers have reported similar findings [2,3].
Good visual acuity, color perception, depth perception, ocular muscle balance are central to good flying performance as 80-85% of all the information processed by an aviator is presented visually. High degree of visual function is important in all phases of flight. Visual standards for aircrew are more stringent than for other branches of IAF. It therefore comes as no surprise that ophthalmologic causes constituted the largest group of disqualifying disabilities.
There were only two candidates who had history of corneal refractive corrective surgeries (LASIK, PRK) and they were declared unfit. Corneal corrective refractive errors reportedly lead to subtle functional visual impairments, which precludes an individual for flying duties [4].
Radiological abnormalities
Radiographs of whole spine, chest radiograph and abdominal ultrasonography are mandatory at initial evaluation of all aircrew candidates.
It was observed in this study that there has been a gradually increasing number of candidates being rejected because of spinal abnormalities/ anomalies detected radiologically. Royal Netherlands Air Force (RNLAF) reported 20% rejections among aircrew candidates due to radiological spinal anomalies [5].
Lumbosacral anomalies (unilateral and bilateral incomplete) alter geometry of spine, and increase chances of disc injury [5], The medical standards at entry stipulate the spinal anomalies/ abnormalities that are acceptable/not acceptable for flying duties. In the present study, congenital anomalies and degenerative spinal conditions were almost equal in number. In an earlier study Bhargava et al. [7] reported a higher incidence of congenital spinal anomalies and lower incidence of degenerative spinal anomalies as compared to the present study (Table 1). Present study included only NDA candidates unlike the study done by Bhargava et al. NDA candidates are from a lower age group and this could possibly explain the slightly lower incidence of degenerative spinal conditions in this younger age group.
Anthropometric incompatibilities
Anthropometry is an important consideration in flying. In the present study, anthropometric incompatibility was found to be one of the leading causes for disqualification. Anthropometric parameters are of immense importance for aircrew-aircraft compatibility and the required standards reflect this aspect. NDA candidates are given waiver if certain anthropometric parameters fall short of the minimum, because of their potential for physical growth. A waiver of 5.0 cm in height, 2.5 cm in leg length and 1.0 cm in sitting height is permissible. Not withstanding the clause for waivers, a large of number of candidates were still rejected.
Otorhmolaryngological conditions. Deviated nasal septum (DNS) and audiometrie hearing loss were the commonest disabilities encountered. Sound functioning of Eustachian tube is essential for equalization of middle ear pressures. This prevents occurrence of otitic barotrauma due to rapid pressure changes involved in flight. DNS may be a cause for compromised functioning of eustachian tube, recurrent infections and compromise of airway. DNS is acceptable after corrective surgery provided no other complications have occurred and adequate airway is ensured.
Hearing is one of the important modes of information transmission in cockpit. Therefore, audiometrie hearing loss is a cause for rejection if it is beyond permissible limits as specified in IAP 430S [1].
Medical conditions. Among abnormalities of the cardiovascular system, ECG abnormalities and cardiac murmurs were the common causes for rejection of candidates. This underlines the importance of meticulous routine examination and investigations. Candidates with ECG abnormalities and cardiac murmurs may have associated organic heart disease. Such candidates undergo careful cardiac evaluation at a specialist centre before being declared unfit.
Electroencephalographic (EEG) abnormalities were cause for rejection among three candidates. In the IAF, electroencephalogram was mandatory for all candidates applying for flying training. Following a policy change in June 2003, unless otherwise indicated, EEG is now carried out only for cadets who are selected for the fighter stream after initial training.
General physical conditions. A candidate is declared unfit if his weight is >20% of the ideal for his age and height. Prevalence of obesity among this late adolescent age group and percentage of obesity among all reported disabilities in NDA candidates is higher than expected and it possibly reflects the problem of obesity in this age group in our general population. Adolescent obesity is an emerging public health problem [8].
Conclusion
Significant numbers of asymptomatic candidates were rejected on medical ground. Ophthalmologic conditions remain the most common cause of rejection followed by spinal abnormalities and anthropometric incompatibilities. Incidence of congenital spinal abnormalities show an increasing trend in this young population group, which is of concern and thus signifies importance of stringent medical evaluation. Physical fitness standards need to be continuously updated in view of current advances in the field of medicine and technology. Periodic retrospective studies analyzing such data are desirable for maintaining high professional standards.
References
- Manual of Medical Examinations and Medical Boards IAP-4303. (3rd Ed (revised)).
- Medical causes of dismissal in candidates selection for pilots in Royal Jordanian Air Force. Aviat Space Environ Med. 2005;76(3):204. (Section 1)
- [Google Scholar]
- An analysis of 375 examinations at Maxwell field for primary flying training. Aviation Medicine. 1936;7:172-76.
- [Google Scholar]
- Excimer LASER photorefractive keratectomy (PRK) for myopia - Present status: Aerospace considerations. Aviat Space Environ Med. 1995;66(7):690-93.
- [Google Scholar]
- Degenerative changes of the spine of fighter pilots of the Royal Netherlands Air Force (RNLAF) Aviat Space Environ Med. 1999;70(11):1057-63.
- [Google Scholar]
- Physiopathology and pathology of spinal injuries in Aerospace Medicine. AGARD-AG-250 (Eng) 2nd ed. Tech, editing and Reproduction Ltd. (London)
- Radiological spinal abnormalities amongst aspiring pilot candidates. Ind J Aerospace Med. 1992;36(2):14-17.
- [Google Scholar]
- Prevalence of obesity amongst affluent adolescent school children in Delhi. Indian Pediatrics. 2002;39:449-52. from the World Wide Web: http://indianpediatrics.net/may2002/may-449-452.htm
- [Google Scholar]




