
Translate this page into:
Effects of simulated prolonged restrained sitting on physical and physiological states

*Corresponding author: Dr T Nepal, MBBS, MD (Aerospace Medicine), Recce and Observation Flight, Indian Army, Chinar Complex, Udhampur - 182101, Jammu and Kashmir, India. docthakur2@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nepal T, Sharma V. Effects of simulated prolonged restrained sitting on physical and physiological states. Indian J Aerosp Med 2021;65(1):38-42.
Abstract
Introduction:
Advancement in aerospace technology, and resultant change in operational capabilities has posed unique challenges on the aircrew, who is required to operate for prolonged periods seated and restrained. Examination of the effects of prolonged restrained sitting on physical and physiological states was the desired objective of the study.
Material and Methods:
Longitudinal evaluation of subjective appreciation of physical discomfort and pain, and physiological parameters, namely, heart rate (HR), blood pressure (BP), oxygen saturation (SpO2), skin temperature, and calf girth changes across 6-h of simulated prolonged restrained sitting was undertaken among 15 healthy male non aircrew volunteers with mean age of 31.2 ± 3.63 years. Subjective discomfort was assessed by Category Partitioning Scale (CPS) and pain by Short-Form McGill Pain Questionnaire (SF-MPQ).
Results:
Prolonged restraint sitting of 6-h resulted in a significant increase in calf girth. Significant changes were also observed in CPS and SF-MPQ scores indicating an increase perception of discomfort and pain. Changes in HR, MAP, SpO2, and lower limb skin temperature were also observed even though these changes were lower in magnitude.
Conclusion:
The pain and discomfort following 6-h of prolonged restraint sitting were found to be appreciable by the subjects. This, along with a significant change in the calf circumference and other physiological parameters were possibly due to effects of venous pooling as a result of sitting for prolonged periods. The effects so observed could have potential flight safety implications and affect mission effectiveness. However, these findings need to be examined in actual cockpit conditions where the seat is more ergonomically designed; yet the aircrew is subjected to a wide spectrum of additional aeromedical stressors.
Keywords
Restrained sitting
Physical discomfort
Category partitioning scale
Short-form McGill pain questionnaire

INTRODUCTION
Modern day fighter aircraft has tremendous operational capabilities in terms of agility, maneuverability, speed as well as endurance. Operational capabilities and endurance of the aircraft have further increased due to induction of mid-air refueling capabilities. With these technological advancements, the aircrew continues to be the limiting factor in terms of physical, physiological and psychological factors. The long duration fighter missions have posed unique aeromedical challenges; even though, the designers have attempted to improve comfort and safety of aircrew. One important challenge in such missions is sitting restrained for prolonged duration of time. In addition, back pain is a known entity in Helicopter flying. Bridger et al. have reported the prevalence of back pain among Royal Navy Helicopter pilots to be 70% which was found to be greatest during instrument flying.[1] In a study by Sharma and Agarwal, 78.9% of pilot attributed the cause of backache to helicopter seat ergonomics, 69.4% to vibrations and 49.4% to poor sitting posture.[2]
Mastrigt et al. studied seat comfort and discomfort on the basis of human context and seat characteristics through a conceptual model framework in a car seat. They reported a correlation between anthropometric variables and seat interface pressure which was affected by body posture. Furthermore, when the driving time increased, the body pressure variables indicated an increase in rating of discomfort implying that the drivers tended to move more frequently when they felt discomfort.[3] De Looze et al. studied the current approaches to ergonomics focused on comfort of sitting[4] which might be due to an increasing amount of time spent while working in sitting posture. They suggested that esthetics could be an indicator for comfort perception, whereas, biomechanics and physiological factors were typically indicators of discomfort.
Games et al. studied 4-h of restricted sitting in an un-padded UH-60 helicopter seat and found a significant decrease in sensibility to touch point pressure on lower limbs, a decrease in skin blood perfusion across time and a 58% decrease in subjective comfort.[5] Subjective discomfort was measured by the Category Partitioning Scale (CPS) and whole body pain was measured by Short-Form McGill Pain Questionnaire (SF-MPQ).[6] Variation of ratings on these scales was found constant and the distribution of rating scores were observed normal. Hence, these scales were reported to be highly reliable and valid for rating discomfort and pain.[7]
With this background, study of physical and physiological parameters during prolonged restraint sitting was considered desirable. Longitudinal evaluation of subjective appreciation of physical discomfort and pain, and physiological parameters, namely, heart rate (HR), blood pressure (BP), oxygen saturation (SpO2), skin temperature, and calf girth changes across 6-h of simulated prolonged restrained sitting was the desired objective of the study.
MATERIAL AND METHODS
Subjects
Fifteen healthy male non aircrew volunteered subjects, aged between 20 to 40 years, participated in the study. An informed written consent was obtained from each participant after explaining the details regarding nature and purpose of the experiment and risks involved. The exclusion criteria were those non-conforming to Indian Air Force anthropometric standards, smokers, and history of backache, any musculoskeletal disease, depression, anxiety, brain injury, and on medications.
Materials
The study was carried out in the existing cockpit chair in the Eye Tracker Laboratory in the Department of Human Engineering at the Institute of Aerospace Medicine, IAF. Necessary modifications of the chair was undertaken by incorporating locally fabricated seat reclining support platform, head rest, and a four-point harness system on the chair. The chair had a fore and aft movement facility. The cockpit had two rudder pedals, an inbuilt throttle and stick, a LED TV as display in front, ideal to carry out simulated flying activities as in a military aircraft. Microsoft Flight software was used to carry out simulated flight during the test. Subjective discomfort was assessed by CPS and pain by SF-MPQ.
Experimentation
The study protocol was approved by Institute Ethics Committee. An informed written consent was taken from all the participants. The participants emptied their bladder and were offered condom catheter/adult diaper as per choice for urination during the experimentation. On the day of experiment, their anthropometric measurements, namely, nude weight, standing height, sitting height, functional leg length, thigh length, head circumference, shoulder width, and calf girth were measured and recorded. The participants donned with flying overall and anti-G-suit and a suitable size aircrew helmet. The fully kitted subjects were secured in seat by the shoulder restraint and tightened by the seat belt at 4 points. Thereafter, HR, BP, and SpO2 were measured. Temperature recordings on anterior and lateral parts of ankle were taken at the duly marked sites. Once seated, the calf girth was recorded. Throughout the test, the shoulder restraint system was kept on locked position even while operating controls. The parameters were collected on an hourly basis for 6 h. The subjects were engaged in simulated flying on a Microsoft flight simulator X and flight controls over a joystick, throttle, and both rudder pedals provided on the LED screen. The participants filled up the questionnaires; CPS and SF-MPQ on an hourly basis. Similarly, calf girth was measured in sitting posture every hour. Water, juices, and snacks were made available on demand during the test. The data collected were pre-test, every hour, and post-test recovery period (30 min following 6 h exposure).
Statistical analysis
Data were checked for normality by Shapiro-Wilk’s IV statistics. Within-subject repeated measures ANOVA was carried out for continuous interval data such as HR, systolic blood pressure (SBP), diastolic blood pressure (DBP), pulse pressure (PP), mean arterial pressure (MAP), arterial SpO2, and records of temperature in the lower limb. Within-subject factors for restrained sitting for eight levels (baseline, hourly data for 6-h, and recovery levels) were analyzed. For all parameters showing significant changes, post hoc analysis was carried out by Tukey HSD. Since the questionnaire scores were ordinal data, non-parametric test Freidman ANOVA was carried out for CPS and SF-MPQ and post hoc analysis by Mann–Whitney “U” test for all significant findings. The level of significance was kept at P < 0.05.
RESULTS
The mean age of the participants was 31.2 ± 3.63 years and the body mass index was 24.2 ± 3.63 kg/m2. Among the anthropometric variables; the mean standing height, sitting height, thigh length, functional leg length, head circumference, and shoulder width were 175.8 ± 4.06 cm, 90.2 ± 3.35 cm, 62.2 ± 1.88 cm, 95.3 ± 6.75 cm, 56.6 ± 1.32 cm, and 45.5 ± 2.26 cm respectively.
A significant decrease in HR was observed across 6-h of restrained sitting. Similarly, PP and MAP also showed significant changes (P < 0.001). The finger SpO2 showed a significant increase across 6-h of sitting (P < 001); whereas, SpO2 on lower limb (2nd Toe, Right LL) showed temporal variation with a mild increase in saturation values. Skin temperature taken at two different sites; one over anterior part of ankle and the other at the posteromedial part of ankle, showed a significant consistent decrease between both the sites across the time. The time difference in temperature was consistent between the two sites, and showed a significant decrease by 1.12 ± 0.69°C on anterior aspect and 1.6 ± 0.79°C on lateral aspect following 6-h of sitting. The calf girth showed a significant increase (+1.4 cm; 3.86%) from baseline compared to 6-h of restrained sitting. Following the recovery period, this increase in calf girth was observed to decrease (0.5 cm; 1.38%). The details are shown in Figure 1.

- Graphical representation of temporal variation in calf girth during prolonged sitting. ***P<0.01, significantly different from baseline, $$$P<0.001, significantly different from 6th h of sitting.
The SF-MPQ response comprised of three scores put together, namely, descriptive scores, visual analog scale (VAS), and present pain intensity (PPI) scores. There was a significant increase in scores of pain and discomfort for all the three subcategories (descriptive scores [F = 7; P = 0.000], VAS [Z = 7; P = 0.000], and PPI [Z = 7; P = 0.000]) across the 6-h of sitting. In non-parametric analysis by Wilcoxon signed-rank test for SF-MPQ, it showed significant variation in descriptive scores (Z = −3.149; P = 0.001), in VAS (Z = −3.432; P = 0.001), and in PPI (F = −3.432; P = 0.001). However, the scores tend to decrease during recovery phase but failed to reach baseline values during recovery. The data are graphically represented in Figure 2.
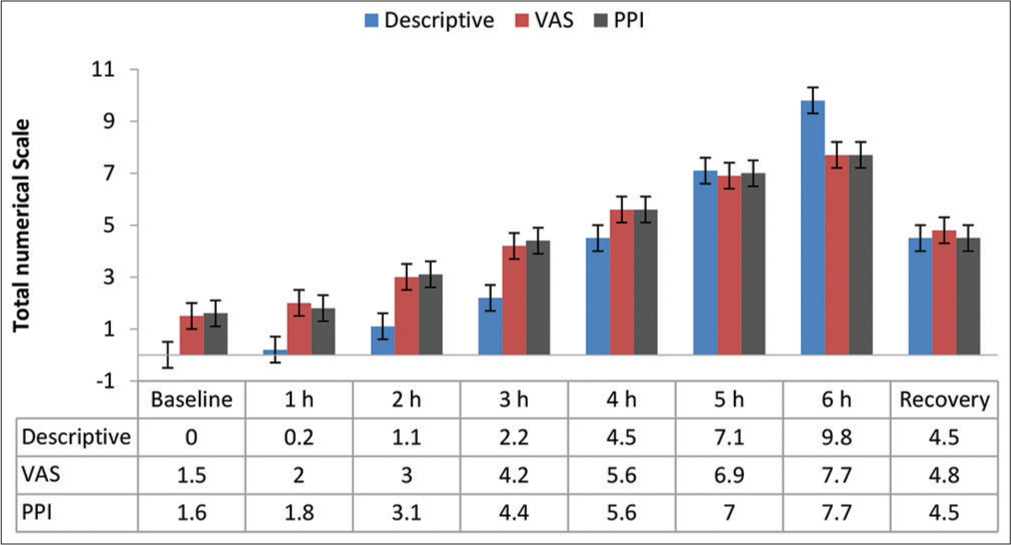
- Graphical representation of Short-Form McGill Pain Questionnaire scores during prolonged restrained sitting.
CPS showed significant increase in discomfort scores as shown in Friedman test (F = 7; P = 0.000) and non-parametric test of Wilcoxon signed-rank test (Z = −3.430; P = 0.001) across 6-h. This is depicted in Figure 3.

- Graphical representation of Category Partitioning Scale (CPS) scores during prolonged sitting.
DISCUSSION
Prolonged restraint sitting is a practical eventuality in military air operations. Our study intended to assess the effects of prolonged sitting of 6-h in a simulated confined and restraint posture on discomfort, pain, and physiological parameters. Most significant results were observed in calf girth, discomfort, and pain scores and mild temporal changes in physiological parameters.
The increase in calf girth (+1.4 cm; 3.86%) from baseline compared to 6-h of sitting could be due to pooling of blood in veins and capacitance vessels in dependent lower limbs on prolonged sitting posture. This fact was further substantiated by the fact that the calf girth tended to normalize (decrease by 0.5 cm; and 1.38% compared to 6-h sitting) following recovery. Pooling of blood in veins of lower limb during prolonged sitting has been well documented by the previous study.[8]
A significantly widened PP from the baseline could be due to the decreasing diastolic and mildly increasing Systolic BP. However, due to mild decrease in SBP and a significant increase in DBP after 2 h of restrained sitting, the PP showed a dip at 3 h and gradual increase to the baseline during recovery. The MAP showed a decrement until 3 h followed by gradual increase to baseline during recovery. This could be explained by the effects of venous pooling of blood and resultant widened PP changes due to decrease in diastolic BP. The overall hemodynamic effects observed are similar to findings by Restaino et al.[9] and point toward pooling of blood in peripheral capacitance vessels.
The results of the study also showed a significant decrease in superficial skin temperature over anterior ankle from baseline values (dT −5°C; 15.7% decrease) and lateral ankle (dT −5.3°C; 17.3%) across 6-h of sitting. It was observed that temperatures recorded over the anterior ankle were slightly higher than the lateral ankle possibly due to pooling of blood in posterolateral side of leg and resultant thermo-radiant loss of heat due to stasis of venous blood. However, there was a significant decrease in temperatures on both the sites during prolonged sitting posture. This could be due to reduction in flow of blood in superficial skin in lower limb on prolonged restrained sitting. Games et al. studied anterior and lateral superficial skin temperature and reported an increase in anterior ankle temperature by 0.61°C during pressure application in buttocks suggesting vascular stasis causing venous pooling and changes during release of pressure.[10] Findings of our study were similar to these observations.
SpO2 level in index finger of right hand of the individual was recorded as a measure of upper limb oxygenation level. The baseline SpO2 of (96.1 ± 1.35%) was found to increase on assuming sitting posture (96.8 ± 0.74%) and following 6-h value (96.6 ± 1.11 %). The SpO2 level in the lower limb (2nd toe right foot) was lower than the upper limb (89.1%), and also increased from baseline (89.1 ± 5.46%) value across restrained sitting for 6-h (92.6 ± 4.09 %). The reasons for changes in SpO2 could not be explained within the scope of the present study.
The discomfort scores were increased on prolonged restrained sitting as measured by CPS. The discomfort scores increased significantly after 2-h of sitting and continued till 6-h. Discomfort scores decreased toward recovery period, however, did not return to baseline immediately. The increase in discomfort levels were pronounced over body locations in neck, back, buttocks, and thigh, indicating seat-man interface interactions and neck loading by additional weight of helmet in the seated posture. The whole-body pain as assessed by SF MPQ score across all time points of assessment showed increasing pain, and a reduction following recovery period. Prolonged restrained sitting, by causing pressure changes over the seat man interface is known to cause pain and resultant frequent posture changes causing distractions and fidgeting.[10] In this study, the pain was mostly localized in cervical region probably due to helmet induced muscular loading of neck muscle and lumbosacral region due to hunched position.
CONCLUSION
The results of the study showed an insight into the possible effects of prolonged sitting of 6-h on physiological parameters and subjective appreciation of pain and discomfort. The pain and discomfort were found to be appreciable by the subjects. This, along with the changes seen on the calf circumference and other physiological parameters, were possibly due to effects of venous pooling as a result of sitting for prolonged periods. The effects so observed could have potential flight safety implications and affect mission effectiveness. However, the findings of the study, need to be examined in actual cockpit conditions where the seat is more ergonomically designed; yet the aircrew is subjected to a wide spectrum of additional aeromedical stressors.
Declaration of patient consent
The authors certify that they have obtained all appropriate consent from the participants.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Task and postural factors are related to back pain in helicopter pilots. Aviat Space Environ Med. 2002;73:805-11.
- [Google Scholar]
- Is backache a serious malady among Indian helicopter pilots: A survey report. Ind J Aerosp Med. 2006;50:13-9.
- [Google Scholar]
- Predicting passenger seat comfort and discomfort on the basis of human, context and seat characteristics: A literature review. Ergonomics. 2017;139:1-23.
- [Google Scholar]
- Sitting comfort and discomfort and the relationships with objective measures. Ergonomics. 2003;46:985-97.
- [CrossRef] [Google Scholar]
- Prolonged restricted sitting eff ects in UH-60 helicopters. Aerosp Med Hum Perform. 2015;86:34-40.
- [CrossRef] [Google Scholar]
- Measures of adult pain: Visual Analog scale for pain (VAS Pain), numeric rating scale for pain (NRS Pain), McGill Pain Questionnaire (MPQ), short-form mcgill pain questionnaire (SF-MPQ), chronic pain grade scale (CPGS), short form-36 bodily pain scale (SF-36 BPS), and measure of intermittent and constant osteoarthritis pain (ICOAP) Arthritis Care Res (Hoboken). 2011;63:S240-52.
- [CrossRef] [Google Scholar]
- Validity and reliability of rating scales for seated pressure discomfort. Int J Ind Ergon. 1997;20:441-61.
- [CrossRef] [Google Scholar]
- Hemodynamic responses in orthostasis following 5 hours of sitting. Aviat Space Environ Med. 1982;53:226-31.
- [Google Scholar]
- Impact of prolonged sitting on lower and upper limb micro and macrovascular dilator function. Exp Physiol. 2015;100:829-38.
- [CrossRef] [Google Scholar]
- Local pressure application effects on discomfort, temperature, and limb oxygenation. Aerosp Med Hum Perform. 2016;87:697-703.
- [CrossRef] [Google Scholar]




