
Translate this page into:
Autokinesis illusion in fighter flying revisited

*Corresponding author: Dr P Sannigrahi, MBBS, MD, Specialist in Aerospace Medicine, Department of Acceleration Physiology & Spatial Orientation, Institute of Aerospace Medicine IAF, Vimanapura, Bengaluru - 560 017, Karnataka, India. drpolash_mrmc@yahoo.co.in
-
Received: ,
Accepted: ,
How to cite this article: Sannigrahi P, Kumar A, Mishra S, Nataraj MS. Autokinesis illusion in fighter flying revisited. Indian J Aerosp Med 2020;64(2):56-61.
Abstract
Introduction:
Autokinesis refers to the perception of motion which is experienced by an aircrew when he fixates his gaze on a stationary point/source of light in an otherwise completely darkened environment. A study was conducted in the Department of Acceleration Physiology and Spatial Orientation, Institute of Aerospace Medicine to determine the time taken for onset of autokinesis in the disorientation simulator (Air Fox DISO) and the effectiveness of various intervention strategies to break the illusion.
Material and Methods:
A total of 103 randomly selected fighter pilots participated in the study. They were briefed about the illusion and the various interventions used to counteract it, such as: (a) Shrugging of shoulders without breaking gaze, (b) stretching of arms without breaking gaze, (c) breaking of gaze for 5 s and (d) breaking of gaze for 10 s (if the illusion is not broken after breaking of gaze for 5 s). Time taken for autokinesis to set in and the effectiveness of the interventions used were noted. Subjective feedback from the participating aircrew was also obtained on their experience on autokinesis illusion in active flying through a structured questionnaire.
Results:
The average time required for onset of the autokinesis illusion in the DISO was observed to be 20.3 ± 15.5 s (range 4.1–121.4 s). Of the 103 aircrew participants, 100 (97.1%) reported that the intervention of stretching of arms was effective, 94 aircrew (91.3%) reported that the intervention of shoulder shrug was effective in breaking the illusion and 99 aircrew (96.1%) were able to counter the illusion by breaking their gaze for duration of 5 s. Autokinesis was experienced in active flying by 17 aircrew, accounting for an incidence of 16.5%. This study reveals that autokinesis involves the interplay of vision, vestibular system, as well as the proprioceptive stimulus in counteracting this illusion. A combination of gaze break and shoulder shrug/arm stretch could be the most appropriate intervention strategy under such circumstances. The operational scenarios conducive for causing this illusion and the physiological basis for the various intervention strategies have been discussed.
Conclusion:
The autokinesis illusion though considered benign has got significant potential for distraction during operational flying. The intervention strategies discussed in the study are effective in breaking the illusion. The pilot community needs to be aware of the preconditions, mechanism, and effectiveness of the intervention strategies in countering this illusion.
Keywords
Spatial disorientation
Autokinesis
Visual illusion
Vestibular system

INTRODUCTION
Spatial disorientation (SD) is an omnipresent threat in aviation, especially in fighter flying. Many illusions have been described in literature which may lead to SD. Autokinetic illusion or autokinesis is one such illusion which refers to the perception of motion which is experienced by an aircrew when he fixates his view on a stationary point/source of light in an otherwise completely darkened environment. It was first observed by von Humboldt in 1799 with respect to apparent wandering of stars.[1] The ideal condition required for autokinesis to occur is the presence of absolute motion, i.e., lack of another visual reference or background. This spatial uncertainty creates the illusion of the stationary light to drift or wander irregularly after some time of inspection.[2] A small dim light, seen against a dark background, is an ideal stimulus for producing autokinesis. After 6–12 s of visually fixating on the light, one can observe it moving at 20°/s or less in a particular direction or in several directions in succession, but there is little apparent displacement of the object fixated. In general, the larger and brighter the object, the less the autokinetic effect.[3] The velocity of the illusory target motion has been estimated to be as high as 10°/s and the total distance “traversed” by the target can range from a few centimeters in central vision to several meters when the target is viewed peripherally.[1] The physiologic mechanism of visual autokinesis is not understood. One suggested explanation for the autokinesis phenomenon is that the eyes tend to drift involuntarily, perhaps, because of inadequate or inappropriate vestibular stabilization, and that checking the drift requires unrecognized oculomotor efferent activity having sensory correlates that create the illusion.[3] Studies by Rucci and Poletti suggest that autokinesis originates from a failure of the visual system in discarding the fixational motion of the retinal image during viewing of an isolated stationary stimulus.[4]
Fighter pilots routinely indulge in “Combat Air Patrol Mission” (CAP) where they are actively looking for any enemy aircraft during their watch hours. In dark night conditions, distant star may appear to move due to “Autokinesis” which may invariably be regarded as an object flying in the sky. Many pilots have reported chasing such moving objects assuming it to be an unidentified aircraft to establish the identity, i.e., friend or foe. Similarly, when a pilot flying at night, following or intercepting another aircraft, perceives another aircraft to be moving erratically when in fact it is not; the unnecessary and undesirable control inputs that the pilot makes to compensate for the illusory movement of the target (due to autokinesis) represent increased work and wasted motion at best and an operational hazard at worst.[3] Autokinesis, though benign in nature, can be a significant distraction in operational flying which may result in SD with serious consequences. Very often, an aircraft in air is diverted to scan a particular geographical area from where another aircraft lost contact and is suspected to be missing. If such a scenario occurs at night, the pilot scans the area in the given coordinates looking for fire and smoke as a sign of crash. If the pilot fixates on a suspected crash site which appears dimly lit solitary light from a distance at night, it may appear to move due to autokinesis. The pilot will invariably ignore such locations and move on to scan other areas assuming the moving light to be some ground features like moving vehicle. This may explain why such missions at night mostly fail. A fighter pilot may have to identify its target from a distance and approach toward it in a bombing mission at night or very early in the morning. The target may appear to move due to autokinesis which may lead to confusion and distraction resulting in increased workload. Following the lead aircraft just by fixating at the tail light in an offensive package in similar scenario may result in “dancing formation” if any of the formation members starts giving control inputs under the influence of “Autokinesis.” Thankfully, such scenario is just a theoretical possibility and has not been reported anywhere in the literature. However, it may lead to some serious consequences, especially in tensed “Op-environment.” During Gulf War II, the US Marines were flying over the Iraqi desert and looked at town lights about 40 km away. The illusory movement of the lights led them to believe that a large combat force was moving out to attack them. They called in an airstrike 15 km away, the estimated position of the lights, which resulted in no enemy assets being destroyed. It was later realized that this misidentification was a result of autokinesis.[5] Autokinesis, more often than not, can have serious consequences in fighter flying. The most commonly used countermeasure is “to shift the gaze” to “break” autokinesis. However, this may not be feasible during operational scenario as pilot may not be able to shift the gaze, namely, during air-to-air refueling, CAP missions or target acquisition, etc. Any additional countermeasures to break autokinesis which are either equally effective or better than shifting of the gaze are likely to be the most appropriate during Ops flying.
All fighter pilots in Indian Air Force mandatorily undergo “Operational Training in Aerospace Medicine (OPTRAM) Course” which includes demonstration of autokinesis illusion in AirFox disorientation trainer. It was observed during the training that the time taken for autokinesis to manifest and effectiveness of the various countermeasures to break the illusion was variable. In view of the above, the present study was conducted to seek an answer to the following questions: (a) Is there any difference in the aircrew who had previously experienced autokinesis in flight than those who have not? (b) Are there any countermeasures which are equally effective or better than “shifting of gaze”? (c) Can the illusion be broken by activating the vestibular or proprioceptive pathway?
MATERIAL AND METHODS
A total of 103 randomly selected fighter pilots participated in the study. They were from various fleets and had reported to Institute of Aerospace Medicine for the OPTRAM course. The AirFox DISO with Stewart platform having six degrees of freedom was used for conducting the study. The protocol was explained and written informed consent was taken from the participants. All the participants answered a preliminary questionnaire to ensure that they did not have any underlying medical conditions or illness. The participants were also informed to refrain from drinking alcohol for 24 h before the day of the experiment and not to consume any medication. Didactic lectures on SD were taken before subjecting the participants to the DISO run.
Autokinesis effect in passive mode was selected for the study in AirFox DISO. The participants were briefed to look toward the dimly illuminated point of light on the DISO screen without making any head movements and to report to the controller if they notice any change in position or motion of the light point. A stopwatch was used for recording the time. The timer was started on starting the effect on the DISO and stopped when the participant reported movement of the light source. The participants were explained about the illusion and also the methods to break the illusion. For the purpose of the present study, the various interventions used were as follows: (a) shrugging of shoulders without breaking gaze, (b) stretching of arms without breaking gaze, (c) breaking of gaze for 5 s, and (d) breaking of gaze for 10 s (if the illusion is not broken after breaking of gaze for 5 s). While “breaking of gaze” is the method commonly used by the pilots to break autokinesis, shrugging of shoulders and stretching of arm would provide the necessary vestibular and proprioceptive inputs to aid in breaking the illusion without breaking gaze. The time taken for initiation of autokinesis was noted on three occasions (namely, T1, T2, and T3), following which the participants were asked to perform any of the intervention strategies described above in random manner to help them getting out of the illusion. The moment they came out of the illusion, a record was made with respect to their subjective feeling of the efficiency of the interventional strategy. On completion of the DISO run, the participants were interviewed with the help of a structured questionnaire enquiring if they had experienced autokinesis during active flying in their respective aircraft and the operational scenario, in which they experienced this illusion.
RESULTS
The mean age, BMI, and flying experience of the participants were 27.2 ± 4.6 years, 23.5 ± 1.8 kg/m2, and 674.5 ± 569.5 h, respectively [Table 1]. The participants consisted of under trainees (UT) pilots, UT operational pilots (UT Ops), fully Ops, and supervisors [Figure 1].
| Role | Number | Age (years) | Mean flying hours |
|---|---|---|---|
| UT | 31 | 23.4±1.3 | 238.97±80.37 |
| UT Ops | 37 | 25.4±1.5 | 438.40±112.02 |
| Fully Ops | 27 | 31.3±3.1 | 1072.22±369.53 |
| Supervisors | 08 | 37.0±1.2 | 2112.5±138.22 |

- Distribution of aircrew participants as under trainees (UT), UT Ops, fully Ops, and supervisors.
The average time required for onset of autokinesis illusion in DISO during three occasions was 24.9 ± 19.2 s (range 7.3– 121.4 s), 17.9 ± 12.1 s (range 5.2–77.4 s), and 18.0 ± 13.2 s (4.1–103.3 s). The overall response was 20.3 ± 15.5 s (range 4.1–121.4 s). As evident from the frequency distribution graph [Figure 2], majority of the aircrew were able to experience the illusory motion within 30 s.
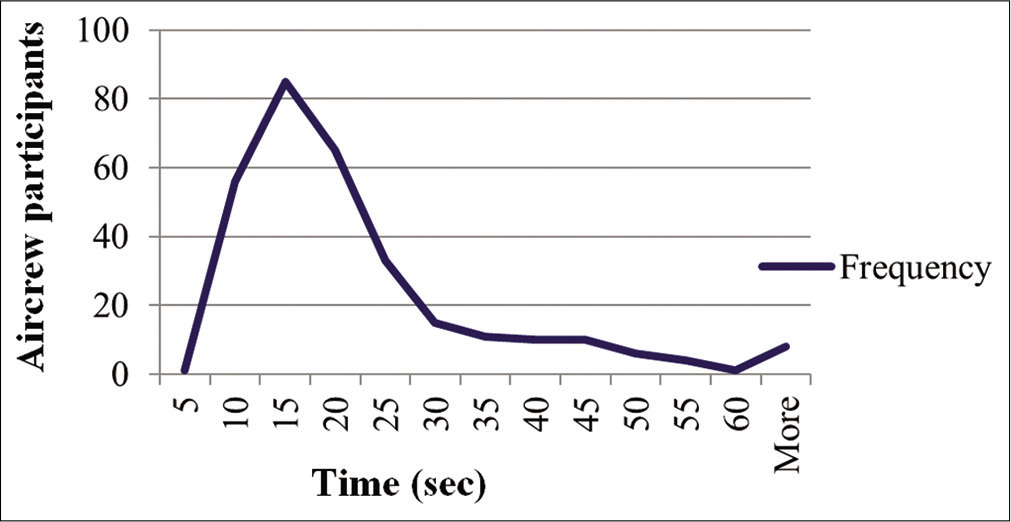
- Frequency distribution of aircrew experiencing autokinesis in DISO.
A comparative analysis was carried out between the autokinesis onset times (namely, T1, T2, and T3) in DISO [Table 2].
| Recording interval | Mean onset time (s) | Comparison | Significance |
|---|---|---|---|
| T1 | 24.9±19.2 | T1 versus T2 | 0.001* |
| T2 | 17.9±12.1 | T2 versus T3 | 0.467* |
| T3 | 18.0±13.2 | T1 versus T3 | 0.0017* |
On analysis of the data received, it was observed that autokinesis was experienced by 17 aircrew (out of 103 participants) during active flying in their respective aircraft, accounting for an incidence of 16.5%. This included 5 UT Ops (13%), 7 fully Ops (25.9%), and 5 supervisors (62.5%). The aircrew had experienced it during air-to-air refueling, dark night sorties over desert, and CAP at night and dark night maritime sorties when they had mistaken a star in the periphery or a static ground light to be another aircraft or adversary and made attempts to join or intercept it. The mean time for onset of autokinesis was analyzed between aircrew who had previously experienced autokinesis in actual flying and those who had not [Table 3].
| Autokinesis onset time | Experienced autokinesis in flying (n=17) | Not experienced autokinesis in flying (n=86) | Significance (P-value) |
|---|---|---|---|
| T1 | 18.1±8.0 s | 26.2±20.5 s | 0.003* |
| T2 | 15.1±8.0 s | 18.4±12.7 s | 0.085 |
| T3 | 15.9±6.9 s | 18.4±14.2 s | 0.138 |
The mean time taken on three occasions for the aircrew who had previously experienced autokinesis were 18.1 ± 8.0 s (range 10.1–33.5 s), 15.1 ± 8.0 s (range 6.6–40.0 s), and 15.9 ± 6.9 s (range 6.8–31.4 s), while the mean time for those aircrew who had not experienced autokinesis was observed to be 26.2 ± 20.5 s (range 7.3–121.4 s), 18.4 ± 12.7 s (range 5.2–77.4 s), and 18.4 ± 14.2 s (range 4.1–103.3 s).
Analysis of the data collected for effectiveness of intervention strategies during the DISO run revealed that out of the 103 aircrew participants, 100 (97.1%) reported that the intervention of stretching of arms was effective in breaking the illusion. Ninety-four aircrew (91.3%) reported that the intervention of shoulder shrug was effective in breaking the illusion and 99 aircrew (96.1%) were able to counter the illusion by breaking their gaze for duration of 5 s. Out of 4 aircrew who could not break the illusion by breaking of gaze for 5 s, 3 succeeded in breaking the illusion after breaking the gaze for 10 s. One participant could succeed in countering the autokinesis only by combining two countermeasures, i.e., breaking the gaze for 5 s and shrugging the shoulders simultaneously. Objectively, it was seen that those aircrew who were able to break the illusion through one intervention method were also able to break it by utilizing the other intervention methods, whereas those who were refractory to one method were refractory to others also and for them, a combination of intervention strategies was found to be effective in breaking the illusion.
DISCUSSION
The onset time for autokinesis has been reported to be 6–12 s.[1,3] However, the overall mean onset time was 20.3 ± 15.5 s and time taken for onset of autokinesis varied from 4.1 sec to 121.4 s. The mean onset time for autokinesis among the participants was significantly higher in the first instance (T1 = 24.9 ± 19.2 s) as compared to the second (T2 = 17.9 ± 12.1 s) and third (T3 = 18.0 ± 13.2 s) instances [Table 2]. This could possibly be due to the fact that most participants had not experienced the illusion earlier and they took time to understand the phenomenon of autokinesis to recognize it and report it 1st time. Subsequent timing reduced due to this familiarity and ability to recognize it [Table 2]. This is also evident with the fact that T1 is significantly different between experienced and inexperienced group, whereas T2 and T3 are not [Table 3]. Hence, with respect to the first question asked in the beginning of the study, our observation showed that there is a difference in the aircrew who had previously experienced autokinesis in flight than those who have not. An aircrew who had experienced the illusion previously in flight are likely to identify it earlier under a similar set of conditions. This finding should be made an important part while imparting training and awareness regarding this illusion.
The time of onset of autokinesis still remains high as compared to what is reported in the literature.[1,3] The pilots with time of onset in excess of 30 s are unlikely to experience it in operational flying as they rarely fixate gaze on any object for this long while flying. Majority of the pilots have time of onset of autokinesis <30 s making them vulnerable during operational flying.
The phenomena of autokinesis have been reported in 37% of US Air Force, 43% of Royal Air Force, and 11% of Indian Air Force pilots.[6-8] The incidence was reported to be 36% (in helicopter pilots) by Tormes and Guedry, 25% by Vinacke, and as 54% by Sipase and Lessard in their respective surveys.[1] In a similar survey of 368 aircrew of the Royal Netherlands Air Force, Pennings et al. found the incidence of autokinesis as 45%.[9] Navathe and Singh carried out a questionnaire survey in 413 aircrew and observed the incidence of autokinesis to be 11% (9.5% in fighter pilots, 7% in transport, and 15% in helicopter pilots) in IAF.[8] The present study on 103 fighter pilots reveals the incidence of autokinesis to be 16.5%, as 17 out of 103 participants had experienced this illusion during active flying. The aircrew experienced autokinesis during various operational scenarios as brought out in the results section. The autokinesis is demonstrated to trainees by their instructors during training sorties as well. They are instructed to avoid prolonged out-the-window fixation by cross-checking appropriate spatial orientation displays at least once every 9 s and preferably more often.[1] However, this may not prevent autokinesis as many pilots have much shorter onset time up to 4.1 s.
Creating awareness among the pilots by demonstrating it on DISO trainer appears to be the best practical solution so that they can identify it on time and institute countermeasures to “break it.” During such training, it is emphasized to the trainee that his gaze should be shifted frequently to avoid prolonged fixation and that a target should be viewed beside and in reference to a relatively stationary structure such as the canopy bow. It was thought that equipping aircraft with more than one light or with luminescent strips to enhance recognition at night may reduce problems with autokinesis.[3] However, the incidence of autokinesis has increased compared to what was reported by Navathe and Singh in 1994[8] and has been reported from operational pilots of modern fighter aircraft with well-illuminated cockpit in this study. It appears that the problem of autokinesis is likely to stay.
The common indoctrination to pilots is to shift their gaze whenever they experience any illusory motion. However, the terminology “shift of gaze” can have different meanings for different persons. Shifting of gaze if associated with head movements in a pilot who is under a somato/oculogyral illusion can lead to Coriolis illusion, and the result could be disastrous. In addition, the time elapsed while changing the gaze by the aircrew is sufficient enough for a target to get out of the sight if it was actually a non-static light source. In view of this, a countermeasure which does not require shifting the gaze is likely to be more operationally relevant. In two methods proposed in this study, the aircrew were specifically briefed not to break eye contact with the light source while they were performing shoulder shrug or arm stretch. These interventions were found to be equally effective as brought out above. Hence, it provides a solution to the second question asked in the beginning of the study with respect to countermeasures which are equally effective or better than “shifting of gaze.” It is important to indoctrinate pilots in all these countermeasures so that they can chose any one of them (or if required, in combination), depending on the operational scenario, to break this illusion.
It has been hypothesized that the illusory motion occurring on fixation of gaze onto a dimly illuminated static source of light against a featureless dark background is due to the involuntary drift of eyes, coupled with inadequate vestibular stimulation (when the pilot is in a prolonged straight and level flight or a prolonged coordinated turn). Hence, the purpose of the intervention strategies performed in our study was to provide vestibular stimulation through activation of vestibulo-spinal tract (by shoulder shrug or arm stretch) and also trigger the vestibulo-ocular reflex (by shifting the gaze).[10] In addition, activities such as shrugging of shoulders and stretching of upper limbs also provided a proprioceptive stimulus, activating the spinocerebellar tract which was helpful in breaking the illusion as mentioned in the results section. However, one pilot could not break the illusion despite using all these measures independently. He was asked to combine shifting of gaze and shrugging of shoulder to break the illusion. This implies that there is a complex interplay of all the orientation cues, namely, visual, vestibular, and proprioception resulting into autokinesis. Autokinesis, like any other SD, is the result of a complex psycho-somato-physiological manifestation which requires deeper understanding.
CONCLUSION
This study reaffirms that autokinesis results due to the complex interplay of vision, vestibular system, and proprioceptive stimulus. It also brings to notice that those aircrew who had experienced the illusion previously in flight are likely to identify it early under a similar set of conditions. The intervention strategies discussed in the study are equally effective in breaking the illusion, through activation of vestibular and proprioceptive pathways. Autokinesis illusion though considered benign has got significant potential for distraction during operational sorties and the pilot community needs to be aware of the preconditions, mechanism, and effectiveness of the intervention strategies in countering this illusion.
Declaration of patient consent
Participant’s consent not required as participant’s identity is not disclosed or compromised in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Visual illusions in flight In: Spatial Disorientation in Aviation. Virginia: American Institute of Aeronautics and Astronautics; 2004. p. :281-32.
- [CrossRef] [PubMed] [Google Scholar]
- Spatial orientation in flight In: Fundamentals of Aerospace Medicine (4th ed). Philadelphia, PA: Lippincott Williams and Wilkins; 2008. p. :168-9.
- [Google Scholar]
- Fixational eye movements and the autokinetic illusion. J Vis. 2009;9:431.
- [CrossRef] [Google Scholar]
- Available from: https://www.dankoboldt.com/space-flight-science-fiction [Last accessed on 2020 Apr 16]
- Spatial orientation and disorientation in flight In: Gradwell DP, Rainford DJ, eds. Ernsting's Aviation and Space Medicine (5th ed). Florida (USA): CRC Press; 2016. p. :286-313.
- [Google Scholar]
- Survey of spatial disorientation in military pilots and navigators. Aviat Space Environ Med. 2003;74:957-65.
- [Google Scholar]
- Prevalence of spatial disorientation in Indian air force aircrew. Aviat Space Environ Med. 1994;65:1082-5.
- [Google Scholar]
- Spatial disorientation survey among military pilots. Aerosp Med Hum Perform. 2020;91:4-10.
- [CrossRef] [PubMed] [Google Scholar]
- Spatial orientation in flight In: Fundamentals of Aerospace Medicine (4th ed). Philadelphia, PA: Lippincott Williams and Wilkins; 2008. p. :155-63.
- [Google Scholar]




