Translate this page into:
Visual Effects of Long Term Active Smoking: Are Aircrew Flying NVG-Aided Missions at a Disadvantage?
Abstract
It is known that smoking reduces visual acuity due to the carbon monoxide content of cigarette smoke & other mechanisms. Since visual acuity with NVGs is already degraded, it is possible that smoking may reduce it further. Aircrew who smoke, may thus be at an additional disadvantage while flying with NVGs. This study aimed to find out whether long term smoking has any adverse effect on visual acuity & field of vision (FOV) through NVGs. 90 subjects (29.3±3.2 yrs) with 6/6 distant vision & N6 near vision participated in this study. They were divided into 3 groups: non smokers, light smokers & heavy smokers. Their blood COHb levels were measured. Using NVGs, their visual acuity was recorded in 3 simulated night sky conditions and FOV was measured. ANOVA was used to find the significance of Snellen VA between 3 groups and Post-hoc Tukey test was used to find the pair wise significance. Kruskal Wallis test with Mann Whitney U test for pair wise significance was used for FOV measurements. The blood carboxyhemoglobin levels were found to be significantly higher in light & heavy smokers (p<0.001) vis-à-vis non smokers. The Snellen visual acuity was also found to be significantly lower in light & heavy smokers in all illumination conditions (p<0.001). The FOV was also found to be significantly reduced in heavy (p<0.001) & light smokers (p<0.05) vis-à-vis non smokers. This study shows that smoking adversely affects visual acuity in light & heavy smokers. This effect lasts for more than 12 hours. Aircrew flying NVG aided missions have an already reduced visual acuity due to the inherent properties of the NVG. This additional decrement in vision could have an adverse effect on flight safety during NVG aided operations.
Keywords
Night Vision Goggles
Smoking
Carboxyhemoglobin
Visual acuity
Field of View

Introduction
The Department of the Army (U.S.) decided to increase night operational effectiveness with night vision devices (NVDs) for use in aviation in 1973 to enhance its night combat capabilities. In the 25 years that have followed, a number of engineering advancements have greatly improved the performance and mechanical packaging of these devices [1]. The Gulf war in 1991 was a landmark event when the whole world became aware of the capabilities of these devices in combat. Experiences in the Balkans and the Persian Gulf have established the utility of night vision goggles in night-time combat.
Major military operations historically have been conducted during daylight when the human visual system is most efficient. Vision is the principal sensory modality with which man gathers information from the external world about him in order to function effectively. The visual system has a total dynamic range in response to light stimulation much greater than any other known photo-detection system. In order to achieve this large dynamic range, several physiological adaptations and compromises have been accomplished. At moderate to high levels of illumination, the cone or photopic system is operational and processes visual information along several dimensions viz color, spatial, and temporal. At lower illumination levels, the rod or scotopic system is operational. The scotopic system integrates light over relatively large retinal areas so spatial resolution is considerably reduced. No color information is processed, and temporal processing is reduced. This limited information provided by the scotopic visual system restricts the capability of the soldier to effectively perform his military duty [2]. Night Vision Goggles (NVGs) are electro-optical image intensification devices that intensify existing light and present a monochromatic intensified image to the user. It is because of this property of NVGs, that they confer a distinct advantage to the user with respect to vision in conditions of low illumination.
Today, night vision goggle aided operations are playing an increasing role in military and civilian aviation [3]. Diverse mission areas and aircraft types are being committed to night operations with an increasing reliance on the use of NVGs. Depending on goggle design, the intensified monochromatic image has a 30-40 degrees circular field of view with a resolution between 20/35 and 20/50 Snellen visual acuity under ideal conditions. As the available light levels are reduced, NVG resolution is reduced to 20/200 or less [4]. Best visual acuity with NVGs is usually 20/40. Given the importance of vision in flying in general, and in night flying in particular, it is evident that aircrew flying NVG-aided missions are at a disadvantage in terms of visual acuity.
Night operations generally require flying at odd hours of the night and can lead to disruption of the body’s normal circadian rhythm. In addition, aircrew need to be at the peak levels of alertness for such missions. Smoking has long been known to be a stimulant of the central nervous system; thus its use in maintaining alertness. Anecdotal evidence suggests that aircrew prefer smoking before a sortie. This could be a matter of habit or an effort to enhance alertness.
Smoking one cigarette results in the saturation of 1-1.5% of the body’s hemoglobin with carbon monoxide [5]. McFarland and co-workers (1944) showed that visual thresholds rise significantly with carboxyhemoglobin (COHb) levels of 2-4 % [5]. Carboxyhemoglobin exerts its effects by reducing the oxygen carrying capacity of the blood, shifting of the oxygen-hemoglobin dissociation curve to the left so that the affinity for oxygen (O2) is increased, unloading of O2 in tissues is impaired and blockade of oxidative phosphorylation . In addition, smoking also affects vision by generation of free radicals and exerting a direct neurotoxic effect on the optic nerve [6].
It has been shown that the smoking of three cigarettes can produce the same total effect on vision as is experienced by ascent to 8000 feet altitude without oxygen [7].
Since visual acuity with NVGs is already degraded to 20/40 due to the inherent limitations of the device, it is possible that smoking may reduce it further. This would imply that a pilot, who is a smoker, is at further disadvantage while flying with NVGs, as far as visual acuity is concerned.
Extensive search of available aerospace medicine literature and the internet (www.pubmed.org) did not reveal any study on effects of smoking on visual acuity through NVGs. Hence, this study was undertaken to determine whether smoking has any effect on visual acuity and Field of Vision (FOV) through NVGs. In addition, correlation between visual acuity with the carboxyhaemoglobin levels was studied.
Material and methods
90 healthy male volunteers, in the age group of 20-35 years (mean age 25.6±3.2) were included in this study. The subjects were divided into three age matched groups of 30 each: heavy smokers, light smokers and non smokers as defined by Centre for Disease Control (CDC) Atlanta (Table 1) [8].
| Smoker | Category definition |
|---|---|
| Current light smoker | Has smoked for 10 or more days in the past 30 days, and has smoked an average of fewer than 5 cigarettes per day in the past 7days. |
| Current heavy smoker | Has smoked for 10 or more days in the past 30 days, and has smoked an average of 5 cigarettes or more per day in the past 7 days. |
| Current occasional smoker | Has smoked for 1 to 9 days in the past 30 days |
| Experimenter | Has either smoked a cigarette or tried or experimented with cigarette smoking, but has not smoked 100 cigarettes and has not smoked in the past 30 days. |
The smoker-subjects had a history of smoking for at least five years [9]. All the subjects had 6/6 (20/20) uncorrected distant visual acuity and N6 near vision. Occasional smokers and experimenters were not included in the study. The study was approved by the Institute Ethics Committee. Written informed consent was obtained from all the participants.
The subjects’ blood carboxyhemoglobin (COHb) levels were measured using the Vankampen and Zjilstra method [10] 12 hours after the last cigarette. The time gap of 12 hours was chosen to enable 3 half lives of COHb to elapse before estimation of blood COHb levels. This method is routinely used at the Institute for estimation of blood COHb levels. It involves comparison of maximum and minimum absorption spectra for a mixture of COHb and haemoglobin. When a solution of oxyhemoglobin is examined in a spectrophotometer, two absorption peaks are observed at 577 nm and 541 nm respectively. The solution of carboxyhemoglobin also shows these bands, but they are shifted towards the blue end of the spectrum with maximum and minimum at 570 and 535 nm respectively. The spectrophotometric analysis of blood was done using the Spectronic® 21 MV spectrophotometer.
The NVG used for this study was a Gen 2++ Aviators Night Vision Imaging System® (New Noga Light (2000) Industries, Ramla, Israel). After re-confirming each participant’s uncorrected distant and near visual acuity, the NVG was focused using the standard NVG focusing procedure followed for the defence helicopter aircrew. The focusing was done in the NVG eye lane of NVG Lab, at the Institute. The eye lane facilitated the requisite distance of 6m (20 ft) and the illumination condition of full moonlight for the focusing procedure. The subjects were made to view the 3×3(Silderman’s) NVG resolution chart from 6 meters with full moonlight illumination on the chart for the purpose of focusing. The visual acuity through NVG was measured using the 1951 USAF Tri-Bar chart (Fig 1) under three different standard conditions of illumination: full moon (0.1 lux), half moon (0.05 lux) and quarter moon (0.01 lux) [11]. The light levels were defined using a diffuse light source in the NVG eye lane, capable of providing an illumination of 0.001 – 0.1 Lux, and were measured using the Research Luxomet-300 FD® lux meter, manufactured by M/S Research Instrumentation Ltd. New Delhi. The Tri-Bar visual acuity values were trigonometrically converted to their Snellen equivalents for ease of interpretation.
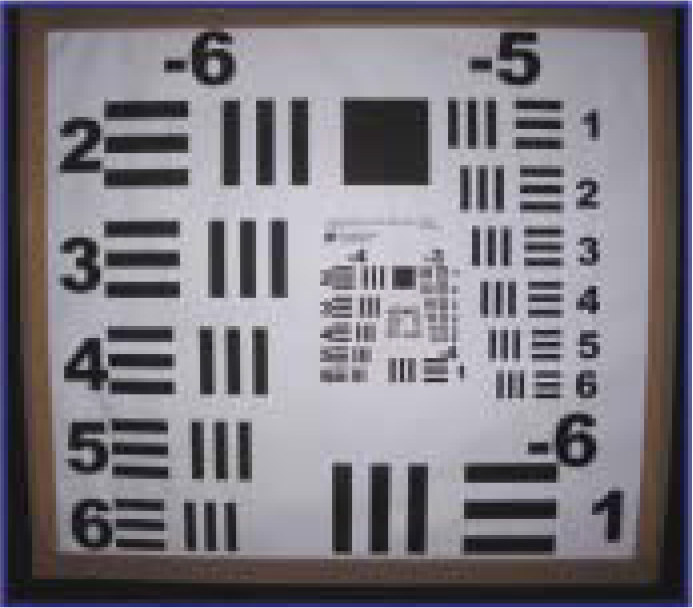
- 1951 USAF Tri Chart
The FOV was measured for all the subjects using a locally designed and fabricated Field of View chart (Fig 2). It had vertical and horizontal bars of 180 cm. length each and was placed at the eye level height. The distances corresponding to various degrees of the field of view were calculated trigonometrically and were marked (as the corresponding values of FOV) on the ground. The subjects, after donning the NVG, were asked to stand facing Fig 2: the chart and then asked to move slowly forward, till the vertical and horizontal bars just abutted the edges of the FOV. The value of FOV was noted for the vertical and horizontal directions.
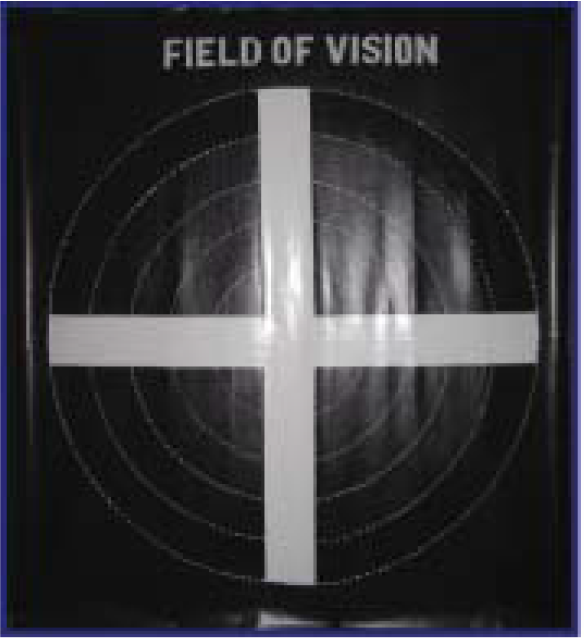
- Field of View Chart
Analysis of variance (ANOVA) was used to find the significance of difference in Snellen VA between the three groups. This was followed by the Post-hoc Tukey test for the pair-wise significance. Kruskal Wallis test for field of view, a non-parametric variables, with Mann Whitney U test for pair-wise significance were used for vertical and horizontal FOV measurements. The linear correlation between blood COHb levels and Snellen VA was derived using Microsoft Excel® statistical software. Significance levels were set at 5 % (p<0.05).
Results
The blood carboxyhemoglobin levels in the three subject groups ranged from 0.59±0.09%, 0.87±0.14% and 1.33±0.30% for non smokers, light smokers and heavy smokers respectively. The increase in carboxyhemoglobin levels was highly significant in light and heavy smokers as compared to non smokers (p<0.001). The significance values are listed in Table 2.
| Heavy/Non smokers | Light/Non smokers |
|---|---|
| <0.001 | <0.001 |
The inter-group significance values for Snellen visual acuity are listed in Table 3 and the mean viewing distances (Snellen visual acuity) are depicted in Fig 3. In full moon illumination, the Snellen VA difference was found to be highly significant between the non smoker group and the light and heavy smoker groups (p<0.001). The difference in the full moon Snellen visual acuity between the light and heavy smoker groups was not significant (p=0.836). In half moon illumination, the difference was found to be highly significant between the non smoker group and the light and heavy smoker groups (p<0.001). The difference in the half moon Snellen visual acuity between the light and heavy smoker groups was not significant (p=0.181). Under quarter moon illumination conditions, the difference was found to be highly significant between the non smoker group and the other two groups (p<0.001). The difference in VA between the light smoker and the heavy smoker groups was also highly significant (p<0.001).
| Illumination | Non/ Light smokers | Non/ Heavy smokers | Light/ Heavy smokers |
|---|---|---|---|
| Full moon | <0.001* | <0.001* | 0.836 |
| Half moon | <0.001* | <0.001* | 0.181 |
| Qtr moon | <0.001* | <0.001* | <0.001* |
Note: *Highly significant P<0.001
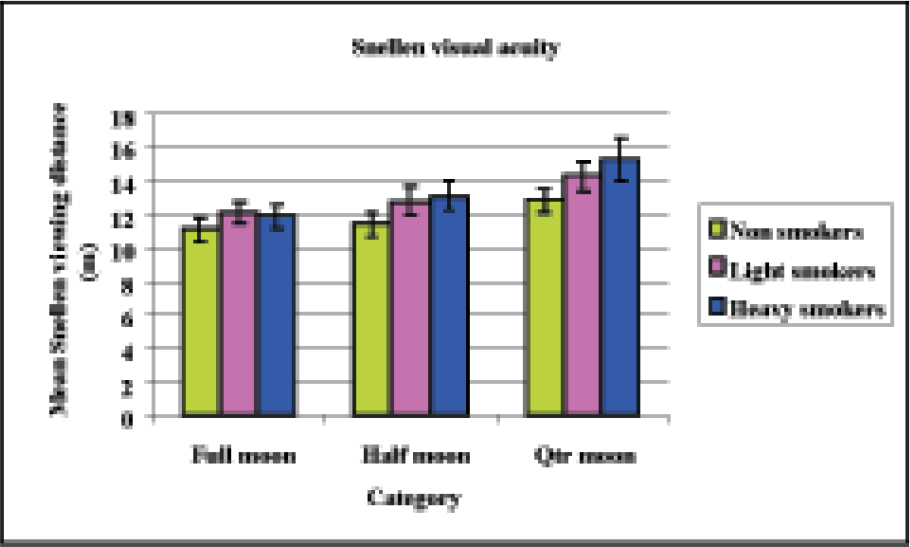
- Snellen Visual Acuity (Mean Viewing Distance)
- Note: Viewing distance is the denominator in the Snellen visual acuity value. It represents the distance (in metres) from which a normal individual views the given line. The values are direct equivalents of Tri-Bar values.
Table 4 lists the inter-group significance values for the three study groups and Fig. 4 depicts the FOV in the three study groups. The reduction in field of vision was highly significant between the non smoker and the heavy smoker groups and between the light and heavy smoker groups in both the vertical and horizontal directions. The difference between the non smoker and light smoker groups was also significant.
| Groups | FOV-Vertical | FOV-Horizontal |
|---|---|---|
| Non/Light smokers | 0.017* | 0.027* |
| Non/Heavy smokers | <0.001** | <0.001** |
| Light/Heavy smokers | 0.002** | 0.001** |
Note: * Moderately significant P<0.01
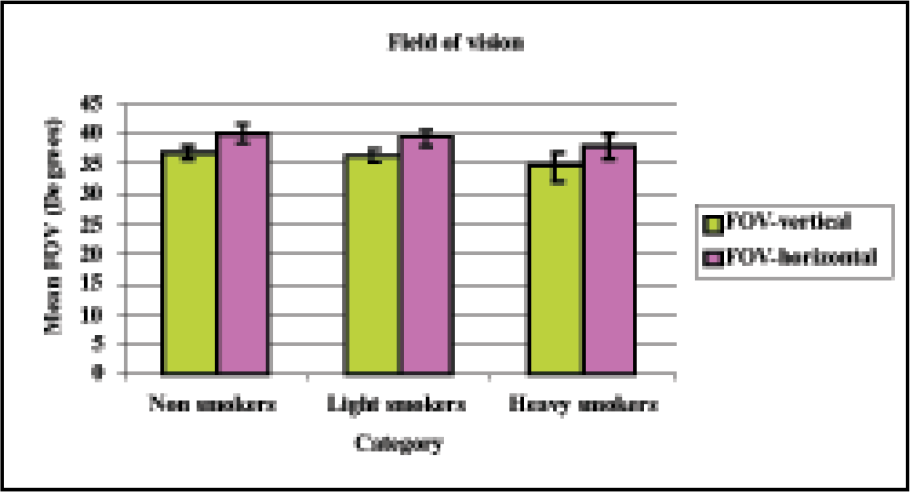
- Vertical and horizontal FOV for the three study groups (Mean ± SD)
A statistically significant positive correlation was observed between blood carboxyhemoglobin levels and visual acuity (Snellen) in heavy smokers under full moon (r=0.49) and half moon conditions (r=0.45). The correlation between COHb levels and visual acuity under quarter moon conditions, although positive, was not statistically significant (Table 5; Figs 5, 6).
| Full moon | Half moon | Quarter moon | |
|---|---|---|---|
| Non smokers | 0.12 | 0.15 | 0.12 |
| Light smokers | -0.34 | -0.16 | -0.02 |
| Heavy smokers | 0.49 | 0.45 | 0.24 |
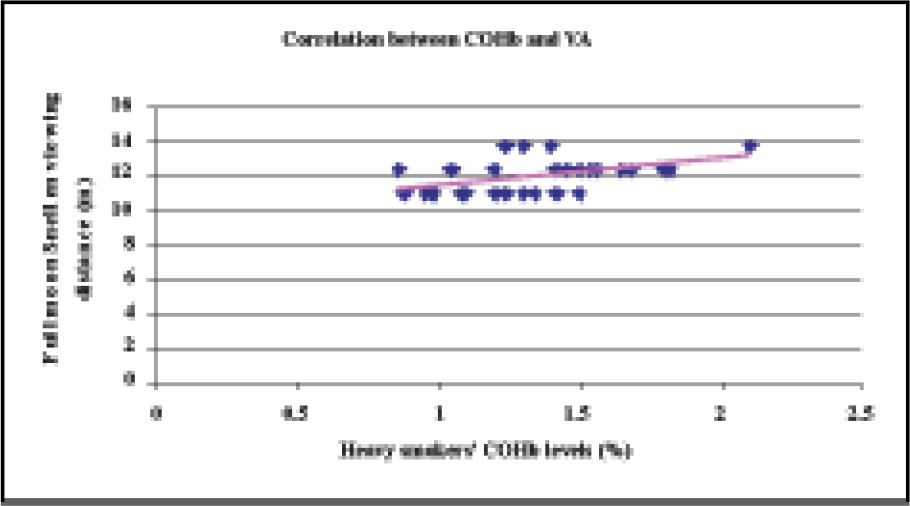
- Correlation between COHb levels and visual acuity for heavy smokers under full moon conditions
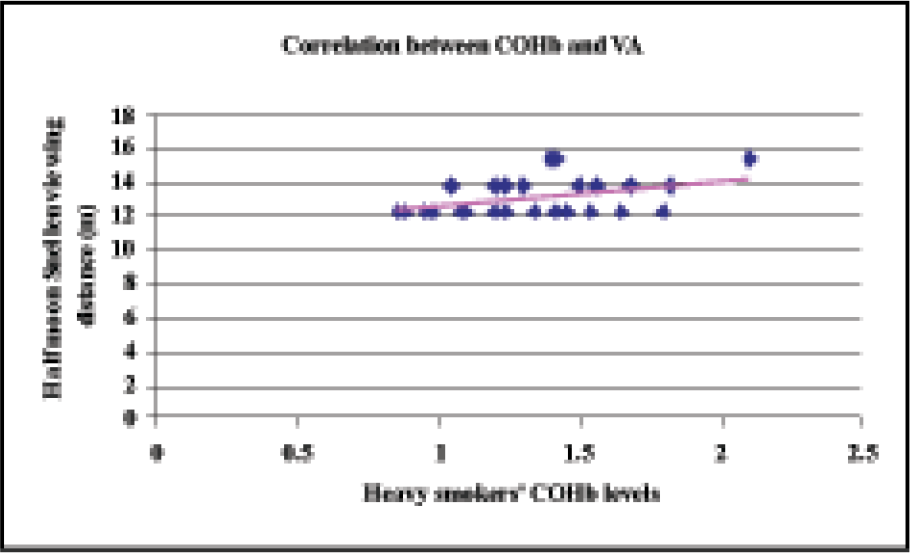
- Correlation between COHb levels and visual acuity for heavy smokers under half moon conditions
Discussion
Various studies have highlighted the adverse effects of smoking on vision, but none have correlated smoking and NVG-aided vision. It is also known that smoking is one of the commonest means of enhancing alertness. Night vision goggles intensify the available light to present a monochromatic intensified image to the user. Although NVG-aided vision is a vast improvement over unaided night vision, it is still not as good as unaided daytime visual acuity. The decrement in visual acuity in smokers may have an additive effect on the already compromised NVG aided vision. Hence, this study was undertaken with an aim to determine the effects of long term smoking on visual acuity through Night Vision Goggles.
Halperin et al showed that the effect of carbon monoxide persists for a remarkably long time. They found that the COHb levels in the blood were around 6.2%, four hours after inhaling carbon monoxide, even when the subjects breathed 100% oxygen and room air alternately for that time period [12]. According to Holbrook [13], the range of COHb found in smokers is 2-15% while the level in non-smokers is near 1%. Dille and Linder [14] did a retrospective analysis of 2660 fatal general aviation accidents and pegged the COHb levels in non smokers at less than 2%. They also reported the maximum levels (10-20%) among smokers. While the results of the present study are in concurrence with these values in case of non smokers, the values for light and heavy smokers have been found to be lower. This can be explained by the fact that the method used for determining COHb levels was different from the methods used in the other studies [5, 12, 13].
The visual acuity through NVGs (Tri Bar and Snellen) was found to decrease with reducing light levels in all the three groups. This is in agreement with an earlier study done by Pinkus and Task [15]. This result also concurs with the observation of De Vilbiss et al [16] who found that under less than ideal conditions, e.g. reduced light levels, incompatible cockpit lights etc, NVG resolution can drop considerably to 20/200 Snellen acuity or lower. The results of this study have not shown such a marked decrement in visual acuity with reducing light levels. The least values of Snellen acuity have been around 6/15 (20/50). The least light levels in which VA was assessed were 0.01 lux (quarter moonlight). It may be possible that NVG visual acuity may fall further if light levels are reduced even more.
It is known that vision through NVGs falls in the mesopic range. In mesopic vision, neither the rods nor the cones operate at peak efficiency, but both actively contribute to visual perception. Connolly et al found that in the mesopic range, mild hypoxia impairs chromatic sensitivity progressively with reducing luminance [17]. The results of the present study establish the fact that smoking degrades visual acuity through NVGs. This implies that smoking and reducing light levels have an additive detrimental effect on VA through NVGs.
The present study also showed a decrement in the field of vision in light and heavy smokers as compared to non smokers. Studies by Hepsen et al [18] and Akarsu et al [19] have shown significant diffuse and localised reductions in visual fields in chronic, moderate to heavy smokers, in both central and peripheral visual fields. They also pointed to the presence of localised scotomas in the central visual fields of moderate to heavy smokers. Horng et al also found a reduction in central and peripheral vision on acute exposure to hypoxia [20]. All these studies were done with automated perimetry. The 40° FOV of the image intensification night vision devices is a theoretical value based on the user being able to place his eye into the exit pupil of the device. Improper adjustment of the helmet attachment can also preclude the aviator from achieving a full 40° FOV [21]. Kotulak reported that the average ANVIS NVG FOV was 36° when the fore-aft adjustment of the helmet mount was set to the maximum-aft position [22]. Hence there is a considerable amount of subjectivity in the assessment of FOV.
The FOV chart used to measure the field of vision in the present study cannot detect focal field losses or scotomas. This method could only give an approximate and subjective estimation of the visual field obtained through an NVG after proper alignment and focusing. Individual variations in the alignment procedure may adversely influence the subjective estimation of the field of view through the NVG. The slight reduction in the FOV observed among some of the subjects may be due to the individual variations in the optical alignment achieved and the consequent subjective estimation of FOV, as all the subjects were inexperienced in NVG use. The use of this FOV chart was a limitation of this study, but because of non availability of standard equipment for testing NVG FOV [Military Specification MIL-A-49425(CR)], its use was resorted to.
The study revealed a positive correlation between increasing COHb levels and Snellen viewing distance for heavy smokers under full moon and half moon conditions. This is in concurrence with other studies on this issue [7, 23]. The correlation between COHb levels and VA was also found to be positive in heavy smokers under quarter moon conditions, but it was not statistically significant.
Conclusion
This study was done with the objective of determining the effect of long term smoking on visual acuity and field of vision through NVGs. The visual acuity through NVGs was found to be significantly reduced in light and heavy smokers, as compared to non smokers. This was true for all the three levels of illumination. In addition, in quarter moon conditions, the visual acuity of heavy smokers was significantly reduced as compared to light smokers as well.
This study proves that smoking has an adverse effect on visual acuity through Night Vision Goggles. This has obvious ramifications on flight safety. Given the operational implications of reduced visual acuity in aviation in general, and in NVG aided flying in particular, the additional decrement in vision because of smoking can jeopardize flight safety and hence, mission accomplishment.
It is recommended that aircrew should be made aware of the effects of smoking on vision and they should be advised not to smoke before undertaking an NVG aided sortie to prevent any decrement in their operational capabilities.
Acknowledgement
The authors sincerely acknowledge the support and guidance given to them by the Commandant, Institute of Aerospace Medicine, Bangalore, the Head of Department, Dept of Human Engineering and the Head of Department, Dept of Aviation Pathology. In addition, the gracious cooperation of all the participants is also acknowledged.
References
- Past, present and future night vision goggles in U.S. Army aviation, RTO human factors and medicine panel symposium Vol 19. San Diego CA: ETATS-UNIS; 1999. p. :1-15.
- [Google Scholar]
- Aviat Space Environ Med. 1994;65:846-850.
- [Google Scholar]
- ‘The Effects of Carbon Monoxide and Altitude on Visual Thresholds’. J Aviation Med. 1994;15:381-394.
- [Google Scholar]
- ‘Dark adaptation of the eye during carbon monoxide exposure in smokers and nonsmokers’. In: Aviat Space Environ Med. Vol 59. 1988. p. :928-31.
- [Google Scholar]
- Aircrew maintenance: Use of tobacco In: Armstrong HG, ed. Aerospace Medicine. Williams and Wilkins; p. :523-524.
- [Google Scholar]
- Advance data from vital and health statistics: Numbers 221–230 Series 16[Web page on the internet] 2006. [Cited 2006 October 14] Available from: http://www.cdc.gov/nchs/data/ad/ad221.pdf Accessed on 14 Oct 06
- [Google Scholar]
- ‘Definitions of subgroups of current smokers. Am J Public 2003 Health. ;93(8):1321-7.
- [Google Scholar]
- ‘The Time Course of the Effects of carbon monoxide on visual thresholds’. J. Physiol. 1959;146:583-593.
- [Google Scholar]
- Nicotine addiction In: Fauci AS, Braunwald E, Isselbacher KJ, Wilson JD, Martin JB, Kasper DL, Hauser SL, Longo DL, eds. Harrison’s Principles of Internal Medicine (16th Edition). McGraw Hill Health Professions Division; p. :2573-5.
- [Google Scholar]
- ‘Effect of tobacco on Aviation Safety’. Aviat Space Environ Med. 1981;52(2):112-115.
- [Google Scholar]
- The effects of aircraft transparencies on night vision goggle mediated visual acuity Proceedings of the 35th Annual SAFE Symposium Phoenix, AZ: SAFE Association, Nashville TN; 1997. p. :93-104.
- [Google Scholar]
- ‘Night vision goggle visual acuity under ideal conditions with various adjustment procedures’. Aviat Space Environ Med. 1994;65(2):705-9.
- [Google Scholar]
- Mild hypoxia impairs chromatic sensitivity in the mesopic range In: Invest Ophthalmol Vis Sci. Vol 49. 2008. p. :820-7.
- [Google Scholar]
- Defective visual field tests in chronic heavy smokers. Acta Ophthalmol Scand. 2001;79(1):53-56.
- [Google Scholar]
- Effects of moderate smoking on the central visual field. Acta Ophthalmol Scand. 2004;82(4):432-5.
- [Google Scholar]
- Visual fields during acute exposure to a simulated altitude of 7620 m In: Aviat Space Environ Med. Vol 79. 2008. p. :666-9.
- [Google Scholar]
- Human factors and safety considerations of night vision systems flight. USAARL Report No. 89-12.
- [Google Scholar]




