Translate this page into:
Relationship of Body Fat with Relaxed G Tolerance
Abstract
+Gz tolerance, like other human physical and physiological characteristics, varies among individuals and is determined by many factors which comprises of both modifiable and non-modifiable ones. One such factor is weight, however weight is itself a composite of fat and fat free mass. The present study was undertaken to study the relationship of body fat, assessed by bioelectrical impedance analysis with relaxed +Gz tolerance. The study was conducted on 30 volunteers with age ranging from 22 to 35 (mean age of 26.2 ± 3.03). The body fat mass was calculated by bioelectrical impedence analysis method and relaxed +Gz tolerance was assessed using high performance human centrifuge at IAM. The data was evaluated using Pearson Product Moment Correlation. The result indicated a significant positive correlation of relaxed +Gz tolerance with body fat mass (p< 0.01). The plausible explanation could be the hormonal changes brought about by the adipose tissue which alter the baroreceptor responses to sympathetic activity.
Keywords
Relaxed +Gz tolerance
Body fat
Bioelectrical impedance

Introduction
For decades, there has been a constant search for the modalities which increase human +Gz tolerance and to identify the factors which could directly affect the inherent tolerance of the human operator. The Aeromedical literature is replete with the factors that have been found to affect the +Gz tolerance. However, there has been no published research on direct correlation of body fat with the relaxed +Gz tolerance.
Tolerance to +Gz level depends upon the rate of +Gz build up. The tolerances to Gradual Onset Rate (GOR) by virtue of allowing baroreceptor reflex mechanism to come into play have been known to be higher than the accelerations where the buildup is at Rapid Onset Rate (ROR).
The baroreceptor responses are innate. Therefore, the relaxed +Gz tolerance (GOR) has been stated to be inherent to an individual (1). Relaxed tolerance of an individual is determined by many factors which comprises of both modifiable and non-modifiable ones. The modifiable factors are the ones which can be avoided so that the +Gz tolerance is not compromised. These include fatigue, drugs, alcohol, less gastric contents, decreased physical fitness, illness and also psychological factors like stress, fear of flying and environmental factors like hypoxia, hyperventilation, high heat loads and dehydration. There are certain non-modifiable factors which affect the +Gz tolerance. These include resting heart rate and blood pressure, age and the anthropometric variables like height and weight (2).
Whinnery in the year 1979 had studied the correlation of anthropometric parameters with the +Gz level tolerance on 59 pilots in the year 1979. He found that shorter and heavier pilots had better +Gz tolerance (3). In a study done by William Lewis Epperson, published in 1980, 24 healthy male participants were subjected to different physical conditioning regimes namely running, weight training. He found that participants who gained weight had improved tolerance for repeated and prolonged exposure to high +Gz loads (4). In another study published in 1986 by KK Gillingham et al, +Gz tolerances of 102 women and 139 men were compared. The analysis identified height had negative influence on +Gz tolerance and weight had a positive influence (5). In 1997, Webb JT et al used correlation and regression analyses to study relationship of +Gz tolerance with anthropometric and physiologic variables on 1,434 fighter pilots. It was concluded by the authors that prediction of +Gz tolerance during centrifuge High +Gz Training is unreliable using anthropometric and physiologic variables (6). In all the above mentioned studies weight is considered as a parameter, however weight (total body mass) in itself is a composite of fat mass and fat free mass (7). Studies conducted on the relationship of relaxed tolerance with these components are very less. Heaps CL et al in 1997, studied relationship of relaxed +Gz tolerance and SACM duration tolerance with Fat Free Mass on 8 females and 10 males. It was found out that Fat Free Mass showed no significant correlation with relaxed tolerance but showed positive correlation with SACM duration tolerance (8). Swetleena in 2009, studied relationship of relaxed and straining +Gz tolerances of 21 female volunteers with their Body Fat Mass which was assessed using skin fold thickness method and no significant correlation was found (9).
The present study was undertaken to study the relationship of body fat, assessed by bioelectrical impedance analysis with relaxed +Gz tolerance.
Material and Methods
The study design was approved by Institute Ethical Committee 30 healthy male fighter pilots of IAF volunteered for the study. Informed written consent was obtained from each participant after explaining the details of the experiment and risks involved. They were instructed to abstain from tobacco and alcohol about 24h prior to the experiment and to avoid coffee and strenuous exercise since morning on the day of experiment. They were also instructed to have adequate sleep on the previous night of the experiment.
Body Fat Mass was assessed using the Bioelectrical Impedance Analysis (BIA) technique. This method measures body fat composition by sending a low, painless, safe electrical current through the body. The current passes freely through the lean tissue, which contains large amounts of water and electrolytes, but encounters resistance when it passes through fat tissue. This resistance to the current is termed ‘Bioelectrical Impedance’, and it is directly proportional to body fat mass. When set against a person’s height, gender and weight, the analyser can then compute body fat mass using predictive equations (10).
Each participant was required to remove their shoes and socks and jewelry. Height and weight measurements were taken as per IAP 4303 (11). The participant would then lay supine on the bed with the arms and legs spreading 30° laterally from midline of their body. The two hands and two feet electrode sites were cleaned with alcohol, and then electrodes were attached at the dorsal surface of following sites: 1) at the imaginary line bisecting the ulnar head, 2) at the 3rd metacarpo-phalangeal joint, 3) at the imaginary line bisecting the medial and lateral malleoli, and 4) at the 3rd metacarpophalangeal joint. Resistance and reactance was measured using instrument, which had been checked for calibration against a SOO-ohm resistor (12). The participants were excused after having the electrodes removed.
High Performance Human Centrifuge available at the Department of Acceleration Physiology and Spatial Orientation in the Institute of Aerospace Medicine was used to give the acceleration profile to the participants. The acceleration profile given to these participants was gradual onset runs with the onset rate of 0.1G/ sec. The participants were made to sit without wearing any Anti G Suit. After making the participants sit and fully strapped up in the centrifuge, the participants were briefed about the dead man’s switch in the gondola and the light bar. By releasing the dead man’s switch the participant can stop the centrifuge run at any time. The light bar consisted of central red light and peripheral green light at 52-56°. The protocol was to start the centrifuge to the basal +Gz level of 1.4G and when the participant is ready, profile is broken and centrifuge accelerates gradually by 0.1 G/sec. The participants were advised to sit relaxed, press the dead man’s switch and hold it in same position, fixate their vision on the central red light which turns on at 1.7G and to keep a lookout for any loss in peripheral green light. On attaining the relaxed +Gz tolerance level, the participant’s peripheral vision starts receding centripetally wherein the participant first notices the loss of peripheral green lights. This is the time the participant is instructed to leave the dead man switch. The +Gz level where the participant leaves the dead man switch is noted and recorded as the relaxed G tolerance level (13).
Descriptive Statistical analysis was applied to obtain mean, SD, kurtosis and skewness. The data was then assessed for normality using Kolmogorov Smirnov test and the correlation between the Relaxed +Gz tolerance and Body Fat Mass was studied using the Pearson Product Moment Correlation.
Results:
30 pilots of age ranging from 22 to 35 with mean age of 26.2 ± 3.03 voluntarily participated in the study. All the participants completed the experiment successfully. None of the participants experienced G induced loss of consciousness. The parameters of only 29 participants were used for analysis due to data loss. The mean Relaxed +Gz tolerance was 4.379 with SD of 0.5926 and mean Body Fat mass was 12.05 kg with SD of 4.089. Details of the same are depicted in table 1 and frequency distribution in figure 1 and 2. The data was subjected to Kolmogorov-Smirnov test and was found to be normally distributed.
| +Gz | Body Fat in kg | |
|---|---|---|
| Min | 3.21 | 5.9 |
| Max | 5.97 | 22 |
| Mean | 4.37 | 12.05 |
| SD | 0.59 | 4.089 |
| Skewness | 0.6 | 0.68 |
| Kurtosis | 0.69 | -0.07 |
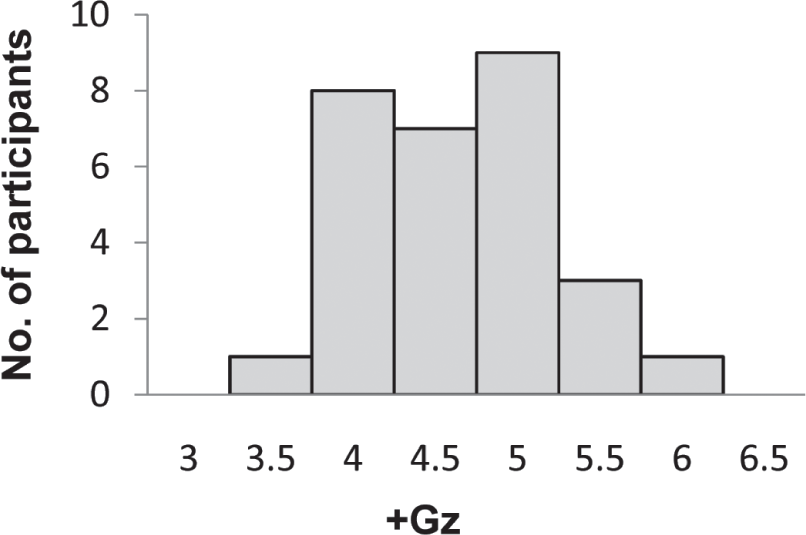
- frequency distribution of Relaxed +Gz tolerance
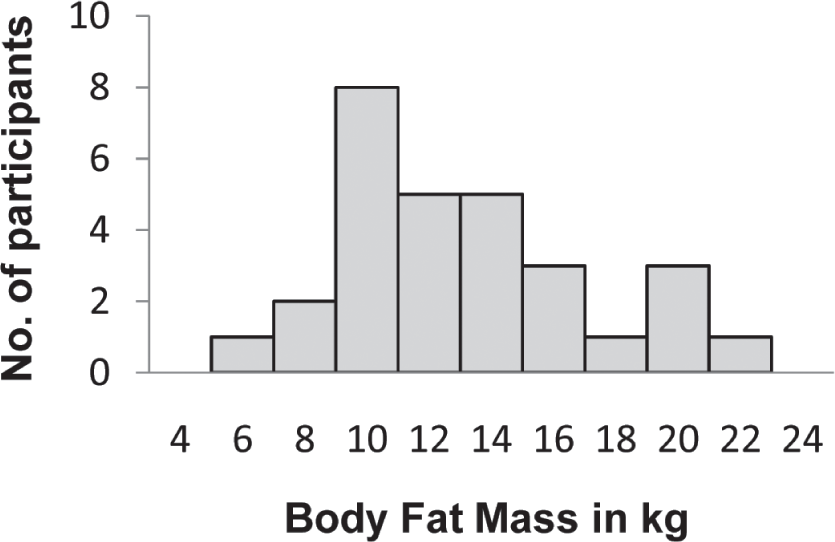
- frequency distribution of Body Fat Mass in kg
The data was then analyzed using the Pearson product moment correlation and a positive correlation of r = 0.473 with high significance of p < 0.01 was found. Same is depicted in table-2.
| Correlation | Relaxed +Gz Tolerance |
|---|---|
| Body Fat in kg | r value – 0.473p value < 0.01 |
Discussion:
In the present study, there was a statistically significant positive correlation between relaxed +Gz tolerance and fat mass. The Pearson’s correlation coefficient (r) was found to be 0.473 which is a fairly positive correlation. The relationship of the Fat mass to +Gz tolerance in the present study is in similar lines with the results by Gillingham KK (6), wherein he had got a significant positive correlation of weight with G tolerance. The studies by Webb et al (7) and Heaps CL et al (8) however showed a similar result wherein the weight had correlated positively but the correlation value (r) never getting more than 0.35. In all of the above studies, weight of the individuals is considered, but weight may not be a very good indicator of the fat mass in the body. Both the fat mass and fat free mass can affect +Gz tolerance in a different manner. In the study by Heaps CL et al, a significant positive correlation of fat free mass with SACM duration tolerance was observed (8). Similar results were found by Weighman et al, who studied relationship of SACM duration tolerance with fat free mass on 10 male participants in 1995 (14). SACM duration tolerance is dependent upon ability to perform AGSM which is in turn dependent on muscle strength and increased fat free mass helps to increase muscle strength (15). However no mention has been made in either of the studies about relaxed +Gz tolerance where fat mass could be a determining factor.
The results obtained from study by Swetleena are contrary to the results obtained in the present study where she found no relationship between fat mass and Relaxed +Gz tolerance. Swetleena in her study has used skin fold measurement method for estimation of body fat mass (9) whereas bioelectrical impedance analysis was used in the present study. The variation could be attributed to method of body fat assessment. Skin fold measurement method requires a considerable amount of technical skill, being meticulous with site location and measurement, and it is difficult to obtain reliable and accurate readings on participants with loose connective tissue or with large fat folds (16). On the other hand, bioelectrical impedance analysis method is devoid of these disadvantages and provides accurate predictions (17). In study conducted by Whinnery, though a positive correlation of weight with relaxed +Gz was found, fat mass did not achieve any significant relationship (3). Once again this can be attributed to fallacies in body fat assessment methods.
Obese individuals are known to possess increased sympathetic nervous system activity when compared to leaner individuals. The possible mechanisms for this could be hormonal changes brought about by the adipose tissue namely, increased concentration of aldosterone, renin and angiotensin II, increased endothelin, decreased adiponectin etc. which increase sympathetic neural activity even at resting state and alter the neural mechanism of baroreceptor responses to sympathetic activity. This effect is more in individuals with excess visceral fat. Higher sympathetic nervous system activity is associated with enhanced sympathetic vasoconstrictor tone. Hence individuals with excess adipose tissue even though they are normotensive have high resting BP than others (18,19) and high resting BP has positive correlation with resting relaxed +Gz tolerance (1). This was the finding in the present study that participants with higher fat mass had a better +Gz tolerance.
Conclusion
The results obtained in this study does propose that relaxed +Gz tolerance is directly proportional to Body Fat, but further studies which consider factors like age, gender and ethnicity with larger sample size are needed to substantiate this finding. The relationship of straining +Gz tolerance and +Gz duration tolerance with body composition also needs to be explored.
References
- AMP working group no. 14, AGARDograph no. 322, 7 Rue Ancelle, 92200 Neurilly-Sur-Seine France: SPS printerLoughton; 1990.
- [Google Scholar]
- Ernsting’s Aviation Medicine. In: David J, ed. Rainford (4th ed). London, England: Hodder Arnold; 2006.
- [Google Scholar]
- +Gz tolerance correlation with clinical parameters. Aviat Space Environ Med. 1979;50(7):736-741.
- [Google Scholar]
- William Lewis Epperson, Effect of physical conditioning on +Gz tolerance, a Doctoral Thesis. University of California, USA March.
- [Google Scholar]
- Unpredictability of fighter pilot G tolerance using anthropometric and physiologic variables. Aviat Space Environ Med. 1991;62(2):128-35.
- [Google Scholar]
- G-tolerance standards for aircrew training and selection. Aviat Space Environ Med. 1987;58(10):1024-6.
- [Google Scholar]
- Exercise Performance and Environmental Stress. Chapter in Exercise Physiology. (6th ed). Baltimore: Williams & Wilkins;
- [Google Scholar]
- Female acceleration tolerance: effects of menstrual state and physical condition. Aviat Space Environ Med. 1997;68:525-30.
- [Google Scholar]
- A study of the relationship between physical fitness and +Gz tolerance among young healthy Indian women [MD thesis] Bangalore: Rajiv Gandhi University of Health Sciences;
- [Google Scholar]
- Electrical impedance in assessing human body composition: the BIA method. Am J Clin Nutr. 1988;47(5):789-92.
- [Google Scholar]
- Manual of medical examinations and medical boards – IAP 4303 (4th edition). New Delhi: Air Headquarters; 2010.
- [Google Scholar]
- The role of anaerobic power in human tolerance to simulated aerial combat maneuvers. Aviat Space Environ Med. 1995;66:938-42.
- [Google Scholar]
- The effectiveness of specific weight training regimens on simulated aerial combat maneuvering G tolerance. Aviat. Space Environ. Med. 1985;56:534-9.
- [Google Scholar]
- Techniques of body composition assessment: a review of laboratory and field methods. In: American Alliance for Health, Physical Education, Recreation and Dance (AAHPERD). 1999.
- [Google Scholar]
- Estimation of body fat in athletes: skin folds vs bioelectrical impedance. J Sports Med Phys Fitness. 2006;46(3):442-6.
- [Google Scholar]
- Sowers Hypertension in Obesity. In: Medical Clinics of North America. Vol 95. 2011. p. :903-17.
- [Google Scholar]
- Sympathetic nervous system behaviour in human obesity. Neuroscience and Biobehavioral Reviews. 2009;33:116-124.
- [Google Scholar]




