Translate this page into:
Lumbar Bar : A Report on two eases
Abstract
A large number of congenital structural abnormalities of the spinal column are incidentally detected during routine radiograph examination prior to selection in aviation duties. Some of the abnormalities although silent in nature, do not affect day-to-day activities in the general population. However, the demanding task and abnormal stresses associated with aviation may prove harmful to the integrity of the spinal column associated with these spinal abnormalities. This paper discusses two cases of Lumbar Bar detected during routine radiograph examination of the spinal column and their aeromedical implication with various stresses associated with flying particularly in high performance aircraft.
Keywords
Lumbar bar
Spondylosis
Lumbar vertebra

Selection procedures involved in selection of candidates and other service personnel for aircrew duties, comprise of thorough physical examination along with investigations including radiological evaluation of the spinal column. During this evaluation, some asymptomatic, congenital conditions are detected which are of vital importance in aviation (1,2).
Congenital abnormalities involving the spinal column are not uncommon in the general population. In the course of time some do become symptomatic, whereas the rest go unnoticed, and are asymptomatic even on severe exertion. Some of the common abnormalities detected on radiological screening of the spinal column are scoliosis, kyphosis, block vertebrae, lumbarisation, sacralisation, Schmorl’s nodes, spondylolysis and spondylolisthesis. Some of these conditions are acceptable for flying duties while others are not (3).
This paper discusses two cases of Lumbar Bar, a rare abnormality of the spinal column detected during routine radiological examination. The condition involves abnormal unilateral bony projection connecting the transverse process of two adjacent lumbar vertebrae. The incidence of the condition in general population is not defined nor is there a laid down aeromedical disposal policy.
It is well known that the spinal column of an aviator is subjected to unusual stress during flight, varying from the usual, sitting in a cramped cockpit, vibration, awkward posture and high Gz, to the exceptional stress occurring during ejection or crash landing. Even aircrew with normal spinal columns report a higher incidence of backache during flying and about 25 to 30% of aircrew sustain compression fractures of the spinal column during ejection (2, 4). Thus any condition that could make the spinal column more prone to injury during the course of the individual’s flying career is a cause for rejection at the time of entry. The aim of presenting these two cases is to discuss the aeromedical significance of such abnormalities detected in candidates for aircrew duties.
Case 1
A 23 years old Sub Lt of Executive Branch, of the Indian Navy reported for medical evaluation for flying duties. He was asymptomatic and general physical examination did not reveal any abnormality.
Routine radiograph examination of spinal column revealed the following findings:
Mild scoliosis of thoracic spinal column with convexity to the Lt side, Cobb’s angle was 07 degrees (acceptable for flying).
Radiograph Cervical Spine - NAD
Radiograph Lumbosacral spine. Prominence of Rt transverse process of lumbar vertebra (LV 3) with a bar of bone attaching transverse process of LV3 with LV2 (Fig-1). CT scan was not carried out. Examination of other systems revealed nothing abnormal. Human engineering evaluation found him anthropometrically and functionally fit for all aircraft. He was thereafter pronounced fit for all aircrew duties.
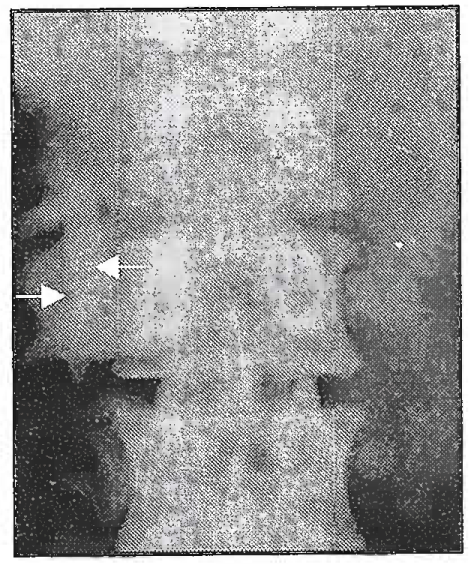
- Fig 1
Case 2
Routine X Ray of Lumbosacral spine of a candidate of 110 NDA at IAM revealed the following abnormalities.
Spina Bifida SVI
Expansion of transverse process of lumbar vertebra 3 on right side with bony out growth connecting the transverse process of LV3 and LV2 on right side. (Fig-2a)
A CT scan showed a linear bar of bone connecting the undersurface of the Rt transverse process of LV2 to the superior surface of the Rt transverse process of LV3. The entire length of right transverse of LV3 was thicker than that on the left side. The bar of bone was not encroaching on the spinal canal or exiting nerve root (Fig-2b).
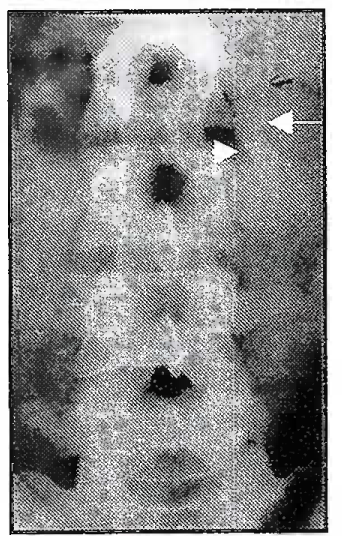
Fig 2a
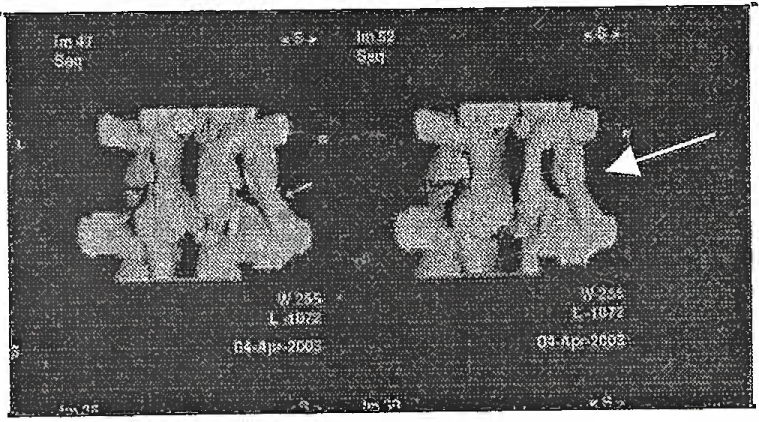
Fig 2b
The candidate was asymptomatic. Systemic examination revealed no abnormalities. On Human Engineering evaluation, spinal evaluation was normal. Anthropometrically he was fit for all aircraft except Iskra on account of sitting height > 90 cm and unfit on Mig 21 Type - 77 with gun sight on account of sitting height > 92 cm.
Radiological evidence of Spina Bifida was not considered to be of any aeromedical significance and hence was acceptable for aircrew duties. He was declared unfit for NDA ( AF) on account of congenital bar of bone connecting the Rt transverse process of LV2 and LV3 associated with other spinal anomalies (Spina Bifida and expanded Rt. transverse process LV3). His final disposal was Unfit NDA (AF), Fit NDA (Army/Navy) on account of Lumbar Bar.
Discussion
The main biomechanical function of spinal column is to transmit the load placed on the body to the supporting structure of the pelvis. The mobility between adjacent vertebrae provides a range of movement along the length of the spinal column. There are two primary curvatures in the thoracic and sacral region, which are present since birth, and two secondary curvatures in cervical and lumbar region due to weight bearing. The load bearing by the spinal column is not uniform because of these curvatures along the spinal axis.
The maximum load is borne by the lower thoracic and upper lumbar vertebra. The functional spinal unit (FSU) defines the functional characteristic of the spinal column. It is a traditional unit of study in spinal kinematics and is constituted by two adjacent vertebrae and their intervening soft tissue (5).
There are primarily three movements of the lumbar spinal column:
Flexion and extension
Lateral bending
Axial rotation
Abnormal kinematics of the spinal column has generally been discussed in response to excessive motion. Subsequently, abnormal kinematics has included restricted motion, abnormal pattern of motion (including abnormal coupling), abnormal distribution of Instantaneous Axes of Rotation (IAR) and paradoxical motion (5).
Amongst the number of relatively common anatomical deformities of the spinal column, one unusual and clinically unimportant is the congenital lumbar rib. This condition occurs more often in females as an asymmetrical structure, which varies in length from few mm to 5-6 cm. Instances in which these anomalous ribs are asymmetrical have been described. They usually present well-formed articulations with transverse process of the first lumbar vertebra. The osseous structure of the rib is normal bone (6).
In the cases described above, there is a similarity with the above condition except for the fact that it arose from LV3 vertebra and was attached to the transverse process of LV2. The presence of this bony structure in continuity with the transverse process of LV2 and LV3 can lead to significant impairment of mobility in that segment of the spine as well as load bearing capacity.
The lumbar bar vertebra functionally, makes that segment of the spine behave like a partial-block vertebra. It can also be considered akin to unilateral sacralisation, a condition disqualifying a candidate for flying (3). The rationale is that the normal FSU transmits loads uniformly through the inter vertebral disc, and it is this transmission of force that would be altered in these cases, leading to increased incidence of spinal compression fracture when exposed to high Gz stress during ejection, crash landing and landing on ground after ejection. The chances of spinal injury, especially lateral compression, will be correspondingly much higher. Similarly during high G maneuvers, the differential lateral stresses could lead to an increased incidence of back pain.
Theoretically the partially fused vertebrae could also lead to reduced mobility of the spinal column, particularly the lateral flexion. But this is of little significance and was not detected on clinical examination of the above two subjects found with this abnormality.
The above response is when the lumbar bar rigidly fuses the FSU. However, if the two vertebrae are connected through a pseudo-arthrosis, the aviation related stresses could make the aviator prone to chronic back pain and abnormal movements across this FSU would also make this region prone to early spondylotic changes.
Conclusion
Lumbar Bar although not common needs to be considered as a specific entity by itself. There are no previous studies to indicate the response of this abnormality to the stresses of aviation nor there are any guidelines as to their Aeromedical disposal. This entity is of aeromedical significance in that aviation stresses like vibration would make the spine prone to chronic back pain as well as early spondylotic changes and the high Gz forces encountered in aviation could make the spinal column more prone to injury.
It is therefore recommended that all cases having radiological evidence of Lumbar bar should undergo CT scan to confirm the extent of the fusion. When so confirmed, such candidates should be considered unfit for flying duties on all types of aircraft.
References
- Radiological spinal abnormalities amongst aspiring pilot candidates. Ind J Aerospace Med. 1992;36:14-7.
- [Google Scholar]
- Congenital abnormalities of spine & flying fitness: Evaluation & Disposal. Ind J Aerospace Med. 2001;45(2):30-36.
- [Google Scholar]
- Indian Air Force Publication 4303 (Manual of Medical Examination). (3rd edition). Section 6.9.1
- Analysis of post ejection spinal injuries - An Indian Experience. Ind J Aerospace Medicine. 1999;43(1):24-28.
- [Google Scholar]
- Part II: Kyphosis; Chapter 1, Physical Properties and Functional Biomechanics of the Spine In: Clinical Biomechanics of the Spine (2nd edition). JB Lippincott Company; 1990. p. :45-59. In:
- [Google Scholar]
- Neuroradiology of the Spine In: Sutton David, ed. Textbook of Radiology and Imaging (6th Edition). New York: Churchill Livingstone Inc; 1998. p. :1489-526. In:
- [Google Scholar]




