Translate this page into:
Evaluation of Cas/Med Evac Facilities in C-17 Aircraft
Abstract
Background:
C-17 aircraft has been recently acquired by India which has the unique quality of being an excellent aircraft for both CASEVAC and MEDEVAC missions. A study was conducted to study the CAS/MED EVAC facilities in this aircraft and a comparison was drawn with IL-76 and C-130 J aircrafts.
Methodology:
Detailed evaluation was carried out on ground in parked C-17 aircraft by studying cargo configurations, patient support facilities in terms of availability of life support systems, oxygen system, power source, equipments availability and through dummy casevac exercise. IL-76 and C-130 J aircrafts were also studied in limited capacity for comparison purpose.
Results:
C-17 is capable of carrying both sitting and lying casualties in different configurations. Cargo compartment equipped with unique Aeromedical Litter stations and utility panel, is capable of supporting lying patients. Seats for sitting patients are cushioned and equipped with backrest and restraint belt. Aircraft contains built-in oxygen system (LOX) and electric power supply through standard US outlets. No other medical equipment is present on-board. Air-worthy equipments will have to be carried separately for critical patients. Logistic support like blankets, linens, etc have to be carried separately.
Conclusion:
The C-17 can utilize small, unimproved airfields in hostile zone. Currently the workhorse in patient transport, the C-17 can be rapidly configured from use as a cargo aircraft into Air Ambulance role. C-17 is a superior aircraft as far as air ambulance role and in flight care is concerned but C-130-J scores higher for scoop and scoot operations.
Keywords
Casevac
Medevac
Globemaster
LOX
Air Ambulance

Introduction
Recently acquired by India, C-17 is a long-range, airrefuellable, heavy logistic transport aircraft; capable of operating into and out of short runways and austere airfields while carrying oversized payloads [1]. The C-17 Globemaster III has the unique quality of being an excellent aircraft for both CASEVAC and MEDEVAC (with enroute medical care) missions. A study was undertaken to evaluate CAS/MED EVAC role of C-17 aircraft and a comparison was drawn with existing IL-76 and C-130 J aircraft.
Methodology
Proposed evaluation was carried out on ground in parked C-17 aircraft. The following methodology was adapted to study various aspects relating to CAS/MED EVAC missions:
Multiple visits were made to visit parked C-17 aircraft, whenever it landed at a forward high altitude base.
Aircraft manuals available onboard were studied.
Multiple interactions were made with aircrew and technical experts.
Static/Dummy casevac trial was conducted on ground.
Certain aspects of IL-76 and C-130 J aircrafts were also studied to draw a comparison with C-17 aircraft.
Following aspects were studied to evaluate the role of aircraft as an air ambulance:
Patient carrying capacity
-
Patient support facility
Oxygen system capabilities for patients
Power supply source for electromedical equipments
Logistics support availability
-
Aeromedical Issues
Noise characteristics
Pressurisation schedule
Environmental control system
Vibration profile
Results
General Characteristics: The aircraft requires a crew of three (pilot, copilot, and loadmaster) for cargo operations. It has a speed of 450 knots at an altitude of 28,000 feet, with an unrefueled range of 2,400 nautical miles (5200 km) and unlimited range with aerial refuelling[2].This aircraft is capable of landing on small, semi prepared runways as short as 3500 feet and 90 feet wide airfield carrying a payload of 72600 kg. Passenger compartment is well lit and equipped with anti-skid flooring (Fig 1).

- Cargo/passenger compartment of C-17
Carrying Capacity of Passengers/Patients: C-17 has carrying capacity of 90 sitting persons (max). It can carry nine lying patients at all times and has the facility to augment it to 36 lying patients. In such case, sitting capacity will vary depending on cargo load, number of medical personnel, type of medical equipments on board, medical condition of patients etc. Usually it can carry maximum of 36 lying and 54 sitting patients (Fig 2). But other configurations are also possible-like nine lying + 90 sitting, 6 lying + 49 sitting patients. Few seats of this seating capacity will have to be kept reserved for medical personnel. Actual carrying capacity may decrease based on crew complement, mission requirements and patient load.
- C-17 in configuration to carry 36 lying patients on 36 litters
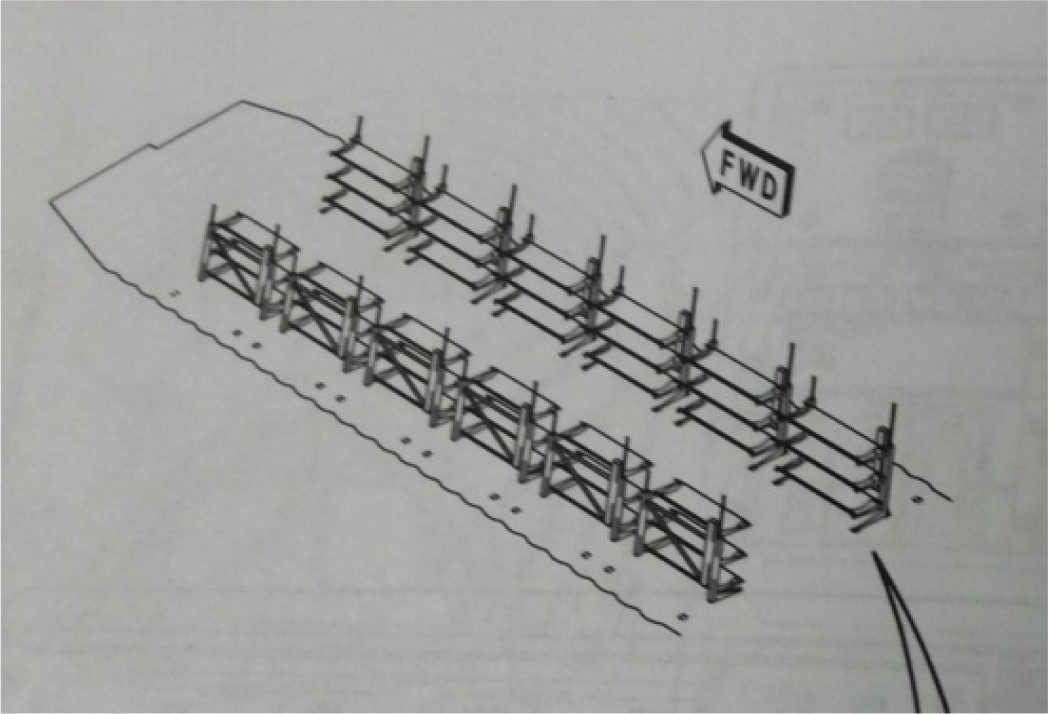
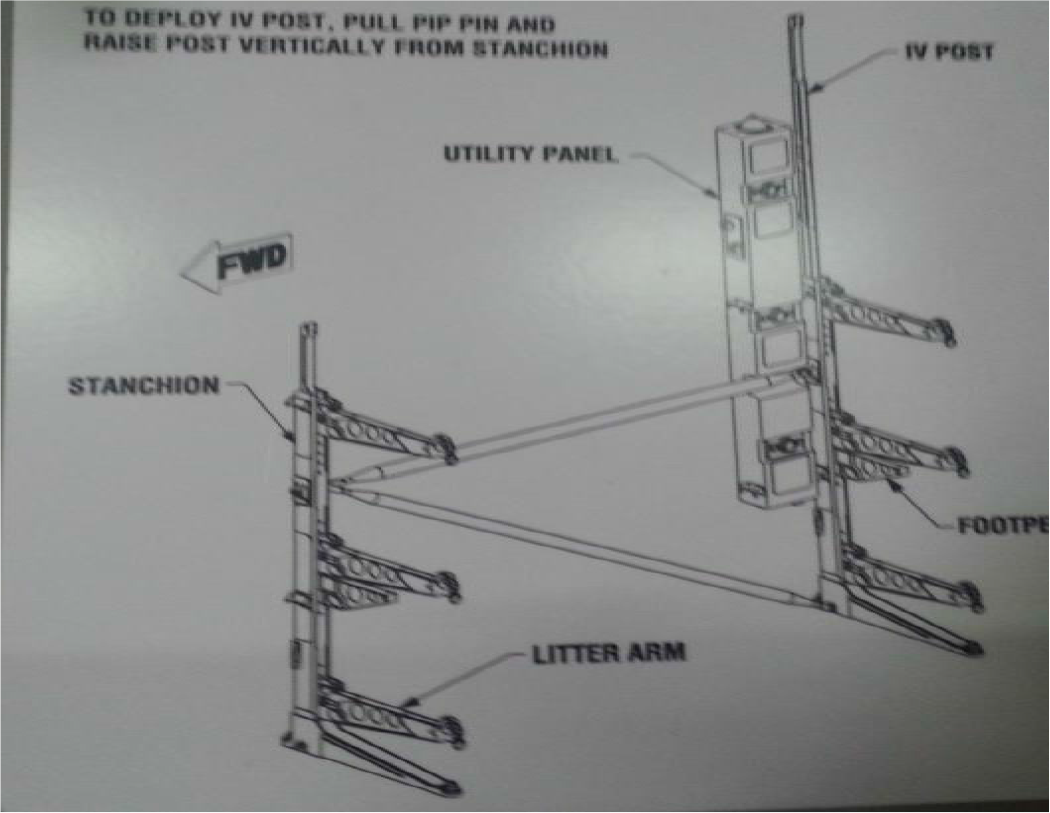
Aeromedical/Litter Stations: C-17 has got three aeromedical stations, each designed to accommodate three litters (Fig 3). One aeromedical station can accommodate three lying patient on three litters. These are stowed permanently in the forward cargo compartment. So at a time this aircraft can carry nine lying patients. Complete installation includes these three litter stations and an additional nine litter stations, for a total of 36 litter positions in the aircraft to carry 36 lying patients. Actual litter spaces may also decrease based upon patient requirements and equipment. A ventilated patient requires one litter tier (3 litter spaces). Characteristics of these litter stations are as described in succeeding paras.
- One aeromedical station with three litters to accommodate three lying patients
Design: The stations have a free-standing design. The litters are supported by horizontal arms attached to vertical stanchions. There are two brackets with locking mechanism on each litter arm to accommodate the handles of stretcher. Each litter has a rated load capacity of 110 kg (250 pounds), which includes the weight of the patient and equipment. Each station has horizontal and diagonal brace to provide support to the stretchers (Fig 3).
Patient Support System: The stations include a utility panel that provides each litter position with a nurse call button, general illumination light and a drop down container and reconfigure the aircraft to required passenger oxygen mask. Pressing the call button turns on a station indicator light on top of the utility panel, a nurse call light at the forward load master station and rings a chime over the public address system (Fig 3). Provisions for each station include structural hard points and electrical and oxygen hook-ups.
Litter Stanchion Augmentation Set (LSAS) Container: C-17 is equipped with LSAS, which is a container like facility to accommodate additional nine litter stations to achieve full capability of carrying 36 lying patients. The door arrangement and interior configuration of this container allows easy in-flight crewmember access to inspect and account the additional nine litter stations needed to maximize the full complement of 36 non-ambulatory patients. One side of the LSAS houses the litter arms and stanchions while the other neatly organizes the diagonal/horizontal braces and utility panels. When an emergency arises and mission directives call for a full complement of litters, the LSAS stands ready to face the challenge. The LSAS can be quickly loaded in the ADS rail system and secured on the ramp ready for immediate airfield departure. The doors, on the 88-inch end wall of the LSAS, can be fully opened to access litter equipment from the LSAS. This makes it very easy for the loadmaster to gain entrance to the container and reconfigure the aircraft to required configuration in-flight. It takes approximately one and a half hours to fully set up the 12 stations needed to accommodate 36 litter (lying) patients (Fig 4).

- LSAS container to carry litters and utility panels
Aircraft Oxygen System
Therapeutic Oxygen Source: A minimum quantity of 75 litres of therapeutic LOX (liquid oxygen) is always available on board. The LOX bottle supply oxygen to pressure demand regulators, recharger hoses, passenger therapeutic oxygen and passenger emergency oxygen system inside the cargo. Oxygen control panel is installed at Load Master Station. An additional quantity of 75 litres of LOX can be carried on demand. There are 12 emergency descent oxygen outlets to accommodate the aeromedical stations, six on each cargo compartment sidewall (Fig 5). In addition, there are five therapeutic or respiratory oxygen outlets located on the right cargo compartment sidewall, allowing oxygen hookup for patients requiring special treatment like ventilatory support. But oxygen masks, hoses, regulators, and other equipment necessary to administer therapeutic oxygen for critical patients are not provided with the aircraft.

- Oxygen outlets to supply aeromedical litter stations
Adequacy: One litre of LOX generates 840 litres of gaseous oxygen. Considering 4-6 litres/min as pulmonary ventilation or 250 ml/min requirement of O2 by body, the quantity appears sufficient for few patients for few hours requiring oxygen enroute. As actual adequacy of oxygen will depend upon conditions of patients, flight time, number of critical patients, it is difficult to comment that actually how many patients can be transferred at a time on oxygen. But definitely 75 litres of LOX appears adequate for 30-36 patients for 2-3 hrs and if augmented with additional bottle of LOX, large number of patients can be transferred on oxygen. Oxygen is administered through oxygen mask of utility panel.
Emergency Portable Oxygen Cylinder
The portable oxygen cylinder is a self-contained protective breathing device to provide oxygen during aircraft decompression, when smoke or toxic fumes are present and to aid in exiting oxygen deficient smoke filled cabins. These are generally to be used by cargo crew in case of emergency descent or for any passenger suddenly falling sick.
Ten of these cylinders are always carried in the cargo compartment. If required these cylinders can also be used for patients (Fig 6).
One cylinder can support one patient for approx 10 min to 1hour. If required this can be kept on litter to administer oxygen to a lying patient.

- Emergency portable oxygen cylinder
Electrical Supply
A primary 115V/60 Hz converter is installed on-board, which provides 60 Hz electrical power to the six aeromedical electrical outlet panels. There are two 115 V AC/60 Hz and 28 Volt DC outlets on each panel. Maximum value of 30 amps is permitted for 60 Hz system (This includes all 60 Hz outlets on the six aeromedical electrical outlet panels).
To increase C-17 electrical amp capability, an Avionics/Unitron Frequency converter may be plugged directly into one of the 115-200V/400 Hz AC outlets located on the six aeromedical electrical outlet panels. Maximum value of 40 amps (20 amps on each side) is permitted when using the Avionics/Unitron Frequency converter.
The connectors are of American type. To connect Indian equipments, suitable adapters will have to be carried as these are not available with the aircraft.
Medical Equipment Availability
Except oxygen system, none of the medical equipments are available with C-17 aircraft. Medical equipments on military aircraft must meet stringent criteria of airworthiness and interoperability. Considering this, critical medical equipments available with our hospitals may not function appropriately unless meeting specific aircraft configurations and tested for airworthiness. In US C-17 have its own airworthy medical equipments which are utilized for MEDEVAC missions.
Stretcher Availability
Presently few stretchers are available with this aircraft which can be loaded on demand. Hospital canvas foldable stretchers may be utilised for casevac. Scoop stretcher is incompatible for litter bracket. The approximate dimensions of stretcher which will be able to fit in litter bracket are as follows:
Length – Upto 78 - 90 inches (6.5 – 7.5 Feet)
Width – 20-22 inches
Handle circumference – 05 inches
Floor Loading of Stretchers
Floor loading procedures for patients can be done for all contingency operations when a time critical environment exists (i.e. non-secure landing zones, hostile area, humanitarian reasons etc.). Stretchers can be positioned side by side or longitudinally on the cargo area floor, with the patient's head towards rear of the aircraft. A total of 48 patients can be floor loaded (Fig 7).
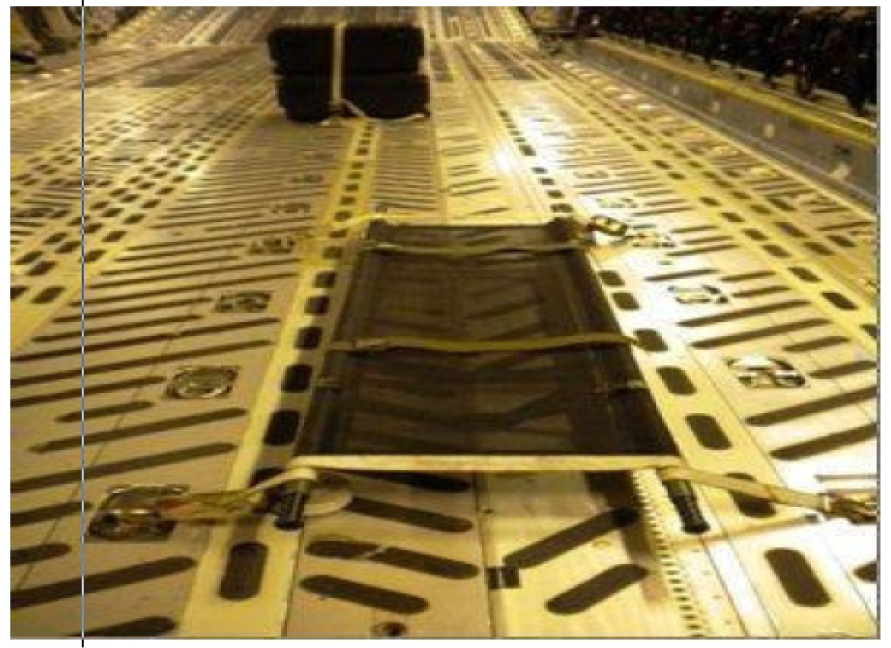
- Floor loading of stretcher
Facilities for Sitting Patients
Seats of C-17 are quite comfortable with backrest. One point harness restraint belt is also available for preventing forward mobility and to restrain the patient. Seats are equipped with life preserver unit which is easy to don during ditching. Oxygen container is available between two seats containing two O masks.
Logistic Support
Items like blankets, pillows, bed sheets etc are not available with the aircraft and will have to be carried separately.
Pressurisation Schedule
Pressurisation mechanism is available and principle of pressurisation schedule is same as in any other pressurised transport aircraft. Aircraft is equipped with state of the art pressurisation control panel capable of maintaining wide range of cabin altitude from sea level to 12000 feet. Depending on aircraft altitude, range of achievable cabin pressurisation is depicted on control panel (Fig 8).

- Pressurisation control panel
Noise Levels
Noise levels of cargo/passenger compartment vary between 85-87 db in various phases of flight which is lower as compared to other aircraft being utilised in similar role. But these levels may still pose problems in communication between medical personnel and patients.
Availability of Trained Crew
India has acquired these aircrafts only recently. C-17 flies with 3 crew - Pilot, Co-pilot and Load Master. They possess basic knowledge of casevac facilities available in aircraft. But neither of them is fully trained in aeromedical evacuation procedures. In US they have separate personnel called Aeromedical Evacuation Crew Members (AECM), who are fully trained in CASEVAC through C-17 and are onboard whenever there is any such requirement.
Comparison
Various characteristics of C-17, IL-76 and C-130 aircraft were compared which revealed superior patient support facility in C-17 aircraft except patient carrying capacity which is more in IL-76 and C-130. C-17 is better equipped for MEDEVAC role and other two appears to be better for scoop and scoot casevac missions (Table 1).

Discussion
C-17 aircraft is equipped with excellent patient support facilities. In different configurations it can carry large number of sitting as well as lying patients. Actual capacity will vary depending on various factors as discussed in results[3].
This aircraft is equipped with unique aeromedical litter stations which are exceptional in terms of patient comfort and medical care. The system of litter stanchions provides 360° access to lying patients (Fig 3). Utility panel on each litter provides patient with personal facilities like light, call button, oxygen mask, electrical hook-ups etc. augmenting in-flight patient care[3]. Overall this system is quite useful in imparting enroute critical care[4].
LSAS container is usually kept reserved, but on demand it is utilised to carry additional litters and helps to configure this aircraft quickly for carrying 36 lying patients[5].
Therapeutic oxygen system comprises of 75 litres of LOX which is sufficient for many patients, and if another bottle of LOX is carried, then oxygen supply becomes unlimited to transfer many patients on oxygen for few hours. This abundant supply of oxygen along with air to air-refuellable characteristics, makes this aircraft suitable even for long range transoceanic missions. Availability of emergency oxygen bottles on board, provides redundancy for in-flight patient management.
Adequate and varied AC/DC electrical power supply is available on board to operate variety of electromedical equipment. Power supply specifications of Indian medical equipment will have to match aircraft electrical configurations. To attain compatibility, the aircraft is provided with suitable adapters to facilitate use of these electrical sockets.
At present, C-17 is not equipped with any electromedical equipment. They need to be carried separately for in-flight medical care. The major testing hurdles before approval for in-flight use, include interface with the aircraft oxygen and electrical systems; assessment of how the device functions across the cabin altitude range of a typical mission (sea level to 8,000 feet) and with rapid decompression to flying altitude; whether the device produces electromagnetic emissions that interfere with aircraft systems; whether electromagnetic emissions from the aircraft interfere with device function; and effect of vibration on the device. Airworthy certification is mandatory for any medical equipment before being utilised for in flight care. Manually operated instruments like Foot Suction pump, Sphygmomanometer for BP monitoring can be utilised. Dry, non-spillable battery operated instruments can be utilised but functioning may still be doubtful. Battery operated portable Pulse Oximeter is a better option to monitor oxygen saturation of critical patient as compared to electrically operated one. Similarly battery operated Automated External Defibrillator (AED) is a better option than conventional Bi-Phasic or MonoPhasic Defibrillator.
As far as logistic support is concerned, few stretchers are carried with aircraft on demand. Hospital stretchers must meet specific dimensions as stated in result, to be able to fit in litter space. Foldable canvas hospital stretchers will generally be compatible. During hostile situation, floor loading technique can be used, in which, stretcher of any dimension can be utilised (Fig 7).
Cushioned seats with backrest and harness are quite comfortable for sitting patients with easy access to oxygen mask and life preserver unit.
This is a pressurised aircraft and as per medical opinion, pilot can maintain wide range of cabin altitudes that can help in better in-flight care of patients. As compared to other aircraft like IL-76 and C-130 J, C-17 is ideal for air ambulance role for carrying out MEDEVAC missions requiring in-flight care.
The other two aircrafts are more suitable for mass casualty evacuation missions. Both C-17 and C-130 J can land on short, semi-prepared runways making them suitable for missions in hostile zones.
Conclusion
The C-17 Globemaster III has the unique quality of being an excellent aircraft for both CASEVAC and MEDEVAC missions. It has characteristic aeromedical/litter stations to carry lying patients and providing in-flight care. The aircraft's interior is well lit and the system of litter stanchions provides 360° access to critical patients. C-17 aircraft contains on-board oxygen system (LOX) that provide abundant medical oxygen at 50 psi.The aircraft offers 115 V/60 Hz AC electric power through standard US outlets, but use of Indian medical equipments will require compatibility and airworthiness certification. Currently the workhorse in patient transport, the C-17 can be rapidly configured from a cargo aircraft into an air ambulance role. The capability of C-17 to utilise small, unprepared airfields, makes it an ideal aircraft for casualty evacuation missions even from conflict zones.
References
- C-17 Globemaster III Technical specifications. Available from URL: http://.Boeing.com/C-17 Accessed on 10 may 14
- [Google Scholar]
- C-17 Globe master III. Available from http://en.wikipedia.org/wiki/Boeing_C17_Globemaster_III Accessed on 10 May 14
- [Google Scholar]
- C-17 Patient Planning Factors, ‘Aeromedical evacuation operations mission planning’. Air Force Instructions 11 2-AE. 3 Available from www.e-Publishing.af.mail Accessed on 05 May 14
- [Google Scholar]
- Wings of Life and Hope: ‘Aeromedical Evacuation’. Problems in Critical Care. 1990;4(4):477-494.
- [Google Scholar]
- ‘Specialty Container Improves C-17 Aeromedical Evacuations. Available from www.airmobilitysystems.com Accessed on 08 May 14
- [Google Scholar]




