
Translate this page into:
Establishment and validation of Institute of Aerospace Medicine-Exercise Maneuver Protocol (IAM-EMP)

-
Received: ,
Accepted: ,
How to cite this article: Dev R, Swamy S, Biswal P. Establishment and validation of Institute of Aerospace Medicine-Exercise Maneuver Protocol (IAM-EMP). Indian J Aerosp Med 2021;65(1):10-6.
Abstract
Introduction:
Musculoskeletal injuries (MSK-I) are among the most common contributors of disabilities worldwide. Aircrew given their charter of duties have a higher risk of developing MSK-I. Functional assessment of aircrew after recovery is conducted at the Institute of Aerospace Medicine (IAM) Bengaluru. The maneuvers utilized in the present assessment lack objectivity and scorability. Hence, this study aimed at establishing an exercise maneuver protocol (EMP), henceforth referred to as IAM-EMP, which could overcome the existing shortcomings.
Material and Methods:
202 age-matched aircrew (180 males/ 22 females) were selected and classified into control (100 healthy aircrew) and experimental (102 aircrew with MSK-I) groups. All aircrew underwent the complete human engineering (HE) assessment. In addition, Functional Movement Screen™ (FMS™) was carried out. Jump test was added to FMS™ after defining its scorability criteria to form the IAM-EMP. EMP was scored on a scale of 0-24. The scores were compiled and analyzed.
Results:
Descriptive analysis showed comparable male and female FMS™ and EMP Scores. Cutoff scores of FMS™ and EMP for the study population were defined using receiver operating characteristic curve analysis. Area under the curve for EMP was found to be statistically better than FMS™ (P < 0.05) in predicting fitness of an aircrew keeping complete HE assessment as gold standard. EMP was validated on randomly selected 50 aircrew (25 from each group).
Conclusion:
IAM-EMP is an objective and scorable tool which can be used on both male and female aircrew between 18 and 45 years of age for their functional assessment post recovery from an MSK-I. Incorporation of the tool with other components of HE assessment would improve the yield of overall evaluation.
Keywords
Musculoskeletal Injury
Functional Movement Screen™
Exercise Maneuver Protocol
Human Engineering
Functional Assessment

INTRODUCTION
The rigors of flying often require an aircrew to endure undue stressors both mentally and physically. Therefore, a higher degree of fitness is desired in an aircrew, both in military and civil aviation vis-à-vis general population, to ensure optimal performance. Aviation stress predispose an aircrew to develop musculoskeletal injuries (MSK-I). Taneja, in a retrospective study involving 626 aircrew, reported that 22.04% of injuries could be attributed to aviation related causes.[1] A significant proportion of injuries are also associated with non-aviation tasks and causes. Gaona reported 67.6% injuries to be non-duty related amongst active aircrew members.[2]
Aircrew with MSK-I in India are subjected to human engineering (HE) assessment at Institute of Aerospace Medicine (IAM) Bengaluru after clinical recovery. The outcome of this assessment helps to certify an aircrew either fit to fly or recommend further observation in a sheltered appointment to ensure functional recovery. The current functional assessment protocol (part of HE assessment) is an impairment-based measure which tests specific joint/ limb function and has the following shortcomings: (a) test results are subjective with significant degree of inter-rater bias, (b) results do not capture graded improvement in function as the test outcomes are either pass or fail, (c) compensatory actions of non-test muscle groups are not considered. To overcome these limitations, a shift to Functional Performance Testing (FPT) model based protocol was desired as it would capture multiple dimensions of function through clustered physical performance movements.[3,4] Functional Movement Screen™ (FMS™),[5,6] a type of physical performance measure has been utilized in various FPT models of functional assessment. Incorporation of FMS™ in the current HE assessment and its validation was therefore intended to be studied.
This study aimed to establish an exercise maneuver protocol (EMP) based on the principles of physical performance measures to assess movement and function in aircrew with MSK-I. The objectives were to make the protocol scorable with an ability to capture improvement in function over time. This testing method was compared with the existing HE assessment protocol for validation.
MATERIAL AND METHODS
Subjects
A total of 208 aircrew consented to participate in the study. Institute Ethics Committee clearance was obtained. The inclusion criteria for enrolling aircrew were as follows: (a) Control group – healthy aircrew with no history of MSK-I in the past 1 year and maintaining unrestricted flying medical category/license. (b) Experimental group – aircrew with history of MSK-I and being observed in non-flying/restricted flying medical category. Participants were excluded if they (a) had a history of intake of analgesics in the past 24 h and (b) were <18 years or >45 years in age.
Equipment
A custom made wooden platform at par with the FMS™ Testing kit was fabricated; it measured 2 × 6 ft with a thickness of 2 inches (inclusive of 5 mm Styrofoam mat pasted atop). In addition, two hollow steel bars measuring 5 ft were used as an indicator stick and hurdle bar. Two steel bars measuring 90 cm with sliding clamps and scale were used to form the hurdle. A standard tape measure was used to record hand length. IAM Anthropometry Platform was used to measure tibial height (required in two of the FMS™ patterns). A 4 ft high wooden platform was used to perform jump test.
Procedure
This study employed a prospective case–control design. Principal worker of the study was FMS™ Level 1 certified. Data were collected between January 2018 and July 2019 in the Department of HE at IAM Indian Air Force Bengaluru. Aircrew were explained the protocol and steps involved in various joint specific exercise maneuvers and FMS™. It was ensured that the aircrew wore appropriate sports rig to prevent any hindrance in body movements. Healthy aircrew underwent HE assessment which includes clinical fitness by the treating doctor, current radiological findings, functional assessment specific to affected limb/joint [Table 1], anthropometry, dynamometry, and range of movement assessment of various joints using goniometry and for spine using Zebris® CMS 20 Spinal Motion Analysis System. Aviation specific stress tests in the form of vibration stress test, high-performance human centrifuge evaluation, and ground cockpit evaluation were undertaken after initial evaluation.
| Foot, ankle and lower leg | Knee | Shoulder | Elbow | Spine |
|---|---|---|---|---|
| Break test | Range of motion test | Apley’s scratch test | Range of motion test | Range of motion test on spinal platform |
| Weight bearing test Toe raise test Hop test Jogging figure of eight test Cut and pivot test Zig zag test Forward/backward test |
Squat test Modified duck walk test Jogging figure of eight test Cut and pivot test Zig zag test Run and jump test |
Shoulder shrug test Throwing test Racket swing test |
Grip strength test Resistive motion test |
Passive straight leg raise test |
In addition, jump test is performed from a 4 ft platform in cases of lower limb and spinal disabilities
The participants completed the seven patterns of FMS™ [Figure 1] thrice;[5,6] highest of the three scores in each pattern was considered to arrive at the final cumulative score. In addition, jump test was also performed. Jump test was scored on a scale of 0–3 in accordance with the principles utilized in scoring the patterns of FMS™. Participants were given a score of 3 when they jumped from a 4 ft high wooden platform with feet joined together and landed without loss of balance, foot movement, and minimal flexion at hip and knee joints. A score of 2 was given to that aircrew who flexed their torso and knee joints before the jump and maintained balance on touch down with up to one step placement to stabilize. A score of 1 was given when aircrew flexed their torso and knee joints before the jump and lost balance on touch down while they were scored 0, if they were apprehensive/refused to jump or reported pain in any part of the body during/ following the jump test. In the experimental group, that is, aircrew reporting for upgradation of flying status after recovery form MSK-I, their clinical and radiological findings were noted. Further, they were subjected to the same protocol of assessment as healthy aircrew.

- (a) Institute of Aerospace Medicine-Exercise Maneuver Protocol Testing Platform, (b) Deep Squat, (c) Hurdle Step, (d) In Line Lunge, (e) Straight Leg Raise, (f) Shoulder Mobility, (g) Trunk Stability Push Up, (h) Rotary Stability, (i) Participant Standing on the Wooden Platform to Perform Jump, (j) Measurement of Hand Length toward Scoring Shoulder Mobility.
FMS™ (0–21) and jump test (0–3) scores were added to derive the EMP scores. EMP was scored on a scale of 0–24, that is, a minimum score of 0 and a maximum obtainable score of 24 when all maneuvers were performed optimally.
Statistical analysis
Type of injury and current clinical and radiological status were the independent variables while outcomes of HE assessment, FMS™ score and EMP score were the dependent variables in this study. Data were compiled and analyzed using Microsoft® Excel 2019 Professional Plus edition and Medcalc® version 19.1.3. Sample size was calculated using G-Power version 3.1.9.4., considering an α error probability of 0.05, power of the study (1-β) 0.80, and effect size of 0.4524 (obtained from EMP data of the study population) for a two-tailed test. Receiver operating characteristic (ROC) curves were plotted for EMP versus current HE assessment and FMS™ versus EMP. P < 0.05 was considered statistically significant and less than 0.01 was considered highly significant.
RESULTS
In all, 202 aircrew (180 males/22 females) fulfilled the study criteria and were included in the study. Hundred healthy aircrew formed the control group while 102 aircrew with MSK-I formed the experimental group. The control group consisted of 90 males and 10 females while experimental group consisted of 90 males and 12 females. The mean age of participants was 28.62 ± 5.13 years (range 22–44 years) in control group and 31.32 ± 5.82 years (range 19–45 years) in experimental group. Age-wise distribution revealed 114 aircrew to be below the age of 30 years while 88 aircrew above the age of 30 years.
Injury-wise distribution amongst the experimental group revealed lower limb injuries to be the most common form of disability (46.08%), followed by upper limb injuries (25.49%) and spinal injuries (24.51%) [Table 2].
| Disability | No. of Participants | Percentage |
|---|---|---|
| Lower limb | 47 | 46.08 |
| Upper limb | 26 | 25.49 |
| Spine | 25 | 24.51 |
| Upper and lower limb | 2 | 1.96 |
| Upper limb and spine | 2 | 1.96 |
Participants in the experimental group underwent the currently utilized joint/limb specific functional assessment protocol in which 97 aircrew were found to be fit while 5 aircrew were deemed unfit. All participants in control group were assessed as fit. In overall HE assessment, 76 aircrew were found to be fit while 26 aircrew were unfit in the experimental group. All aircrew in control group were fit.
All participants were subjected to FMS™ protocol and cumulative scores plotted against outcomes of HE assessment [Figure 2]. Median score in control group was 17 (95% CI for median 17–18) while that in experimental group was 17 (95% CI for median 16–17). Gender-wise distribution of FMS™ scores was found to be similar among male and female subjects [Figure 3]. In addition, the aircrew were scored for the jump test. These were added to FMS™ scores to arrive at EMP scores. Median EMP score in control group was 20 (95% CI for median 20–20, range 16–23) while that in experimental group was 19 (95% CI for median 19–20, range 6–24). EMP cumulative scores were plotted against outcomes of overall HE assessment for both control and experimental groups [Figure 4]. Trend in scores amongst both the groups were found to be similar. Gender wise distribution of EMP scores were found to be similar amongst male and female participants [Figure 5].

- Functional Movement ScreenTM scores among aircrew in control (blue) and experimental (orange) groups.

- Gender-wise distribution of Functional Movement ScreenTM scores in the entire study population.

- Exercise Maneuver Protocol scores amongst aircrew in control (blue) and experimental (orange) groups.

- Gender-wise distribution of Exercise Maneuver Protocol scores in the entire study population.
The total study population was divided into two parts of 152 and 50 (25 each randomly sampled from control and experimental groups) participants. 152 participants (75 in control and 77 in experimental group) were used to establish the cutoff value for classifying functional fitness using ROC curve analysis of EMP composite scores against outcomes of overall HE assessment. A cutoff score ≥18 was obtained with an area under the curve (AUC) of 0.886 and an associated Youden Index of 0.6816. Sensitivity and specificity of EMP at this score were 82.44% and 85.71%, respectively [Table 3]. Pairwise ROC curve comparison of FMS™ and EMP composite scores showed significant statistical difference in AUC (P = 0.0285) [Figure 6].
| Criterion | Sensitivity | 95% CI | Specificity | 95% CI | +LR | –LR |
|---|---|---|---|---|---|---|
| ≥6 | 100.00 | 97.2–100.0 | 0.00 | 0.0–16.1 | 1.00 | - |
| ≥15 | 100.00 | 97.2–100.0 | 23.81 | 8.2–47.2 | 1.31 | 0.00 |
| ≥16 | 97.71 | 93.5–99.5 | 28.57 | 11.3–52.2 | 1.37 | 0.08 |
| ≥17 | 91.60 | 85.5–95.7 | 61.90 | 38.4–81.9 | 2.40 | 0.14 |
| ≥18 | 82.44 | 74.8–88.5 | 85.71 | 63.7–97.0 | 5.77 | 0.20 |
| ≥19 | 60.31 | 51.4–68.7 | 90.48 | 69.6–98.8 | 6.33 | 0.44 |
| ≥20 | 32.82 | 24.9–41.6 | 100.00 | 83.9–100.0 | - | 0.67 |
| >24 | 0.00 | 0.0–2.8 | 100.00 | 83.9–100.0 | - | 1.00 |

- Pairwise comparison of receiver operating characteristic curves of Functional Movement Screen™ and Exercise Maneuver Protocol considering outcomes of overall HE assessment as standard.
EMP cutoff score was applied on the scores obtained by the randomly sampled 50 participants for validation. There were 45 participants who were fit on overall HE assessment and 5 were unfit. EMP classified 43 participants as fit and 7 as unfit [Figure 7]. It was observed that four aircrew scored 17 each on EMP of which two were fit and two were unfit on HE assessment. A 2 × 2 contingency table analysis revealed EMP to be highly specific (100%) and sensitive (95.5%) with a positive predictive value of 100% and negative predictive value of 71.4%.
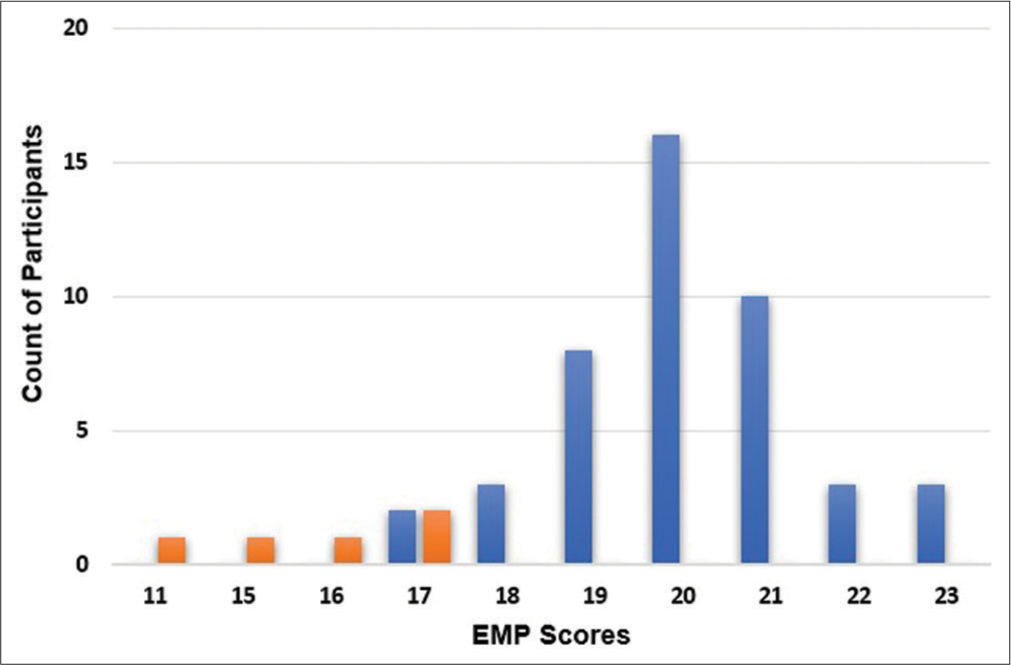
- Exercise Maneuver Protocol composite scores of the randomly selected 50 participants. Subjects found fit (blue) and unfit (orange) in HE assessment are depicted.
DISCUSSION
Aviation related tasks and stressors make the aircrew susceptible to develop MSK-I.[1,2,7,8] Restrained sitting in a closed confined workspace for prolonged hours has shown to cause early development of spinal disabilities. Low back ache is one of the most common disabilities which aircrew suffers. In addition, indulgence in sports activities makes them susceptible to develop limb injuries. The initial disposal of such injury is focused on treatment and rehabilitation. On recovery, HE assessment is carried out to assess level of fitness. The currently utilized joint specific functional assessment protocol plays a major role in evaluating an aircrew following recovery from MSK-I. The tests in the protocol are derivatives of clinical methods and partly assess functional state. The result obtained in this study is a testimony to the same as the existing protocol could correctly identify only five of the 26 aircrew who were found unfit in overall HE assessment. Twenty-one aircrew found fit using the existing protocol could not tolerate the aviation specific stress tests.
Physical performance measures or physical competency testing assess overall function of the body. Such testing has been used in the field of sports since the early 2000s to ascertain an athlete’s level of fitness. This assessment is usually done before athletes resume participation in sporting activities after recovery from an injury.[5,6,9] The nuances of flying and associated aviation stressors require the aircrew to maintain highest level of fitness standards. Such fitness levels justify their comparison to athletes associated with various sports. Hence, it was considered to use a similar model of testing for the aircrew population.
FMS™ has been widely used in the field of sports and occupations to assess an athlete’s/serving personnel’s physical performance before their return to active sports or duty.[5,6,9-13] The screen captures symmetric and asymmetric body movements through seven exercise patterns (each of which are scored on a scale of 0–3). A score of 0 is defined as a painful response in any part of the body during a movement pattern while a score of 3 illicit correct responses. The maximum score an individual can achieve on FMS™ is 21 while minimum is 0. Cumulative scores ≥ 14 in general population have been considered as functionally fit.[5,6,9] However, population specific cutoff scores exist to classify an individual’s fitness.[11,12,14-16] FMS™ patterns were studied visà-vis present testing protocol. It was noted that FMS™ could capture all the movements involved in various maneuvers presently utilized except the biomechanics involved in jump. In addition to the joint movements, impulse forces/jolts are imparted to the body on ground impact in a jump which FMS™ does not emulate. Hence, it was considered to add Jump test to FMS™ after defining its scorability criteria, thereby forming a new scorable scale called EMP.
The number of female participants in the study was low compared to males. This was expected as it is representative of the proportion of females in aircrew population. Based on the ROC curve analysis, a score of ≥18 attained on the EMP was established as the cutoff for the normal aircrew. FMS™ and EMP scores were similar amongst male and female participants; this result was similar to the findings observed in the studies by Kiesel and Schneiders.[9,16] At similar specificity (85.71%), EMP scores were found to be more sensitive (82.44%) than FMS™ scores (68.70%) in predicting the fitness of HE assessment. EMP scores in control as well as experimental groups were found to be similar. This finding implies that an aircrew who has recovered from an MSK-I are expected to perform functionally like a normal aircrew.
Results obtained on validation of EMP using a random sample of 50 aircrew were better than the expected sensitivity and specificity of EMP as defined by ROC curve analysis. EMP cutoff score of ≥18 could correctly classify aircrew as functionally fit or unfit irrespective of their clinical or radiological status. Compared to existing functional assessment protocol, IAM-EMP would add value and increase the yield of overall HE assessment.
Apart from the ability to classify fit and unfit aircrew, the IAM-EMP presents a functional assessment protocol which is scorable at four levels, is objective to a large extent, is standardized to avoid inter rater variability, and can be used as a tool for follow-up in case of aircrew who are found unfit during the current evaluation.
This study is validated for use in aircrew who are up to 45 years of age. The low proportion of older aircrew in the study is a reflection of similar proportions among the actual flying aircrew in military flying. The cutoff values found in this study may not be suitable for an older aircrew population who are expected to have a lower score.[17] However, in their case, their large experience in flying may compensate for their lower score to allow a flying category. A separate study may establish the cutoffs for that population.
CONCLUSION
The current scheme of HE assessment for aircrew with MSK-I is comprehensive. However, due to lack of a testing component which adheres to the principles of physical performance measures, it does not fulfill the criteria needed to qualify as an FPT model. Replacing the existing functional assessment protocol with IAM-EMP would overcome this limitation thereby making HE assessment more objective and repeatable.
Acknowledgment
The authors would like to thank Gp Capt (Dr) YS Dahiya, Senior Advisor (Aerospace Medicine) for having envisioned the requirement of such a protocol and having given the study its current direction.
Declaration of patient consent
The authors certify that they have obtained all appropriate consent from the participants.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A retrospective analysis of musculoskeletal disabilities in military and civil aircrew. Ind J Aerosp Med. 2008;52:8-13.
- [Google Scholar]
- Comparative study of musculoskeletal injuries in transport aircrew. Aviat Space Environ Med. 2010;81:688-90.
- [CrossRef] [Google Scholar]
- The assessment of function: How is it measured? A clinical perspective. J Man Manip Ther. 2011;19:91-9.
- [CrossRef] [Google Scholar]
- The assessment of function. Part II: Clinical perspective of a javelin thrower with low back and groin pain. J Man Manip Ther. 2012;20:83-9.
- [CrossRef] [Google Scholar]
- Pre-participation Screening: The use of fundamental movements as an assessment of function-Part 1. N Am J Sports Phys Ther. 2006;1:62-72.
- [Google Scholar]
- Pre-participation Screening: The use of fundamental movements as an assessment of function Part 2. N Am J Sports Phys Ther. 2006;1:132-39.
- [Google Scholar]
- Investigation of self-reported musculoskeletal injuries on post-deployment health assessment forms for aeromedical evacuation personnel. Mil Med. 2015;180:1256-61.
- [CrossRef] [Google Scholar]
- Can serious injury in professional football be predicted by a preseason functional movement screen? N Am J Sports Phys Ther. 2007;2:147-58.
- [Google Scholar]
- The effect of an intervention program on functional movement screen test scores in mixed martial arts athletes. J Strength Cond Res. 2015;29:219-25.
- [CrossRef] [Google Scholar]
- Functional movement screen as a tool for functional evaluation and prediction of the risk of injury among floorball athletes. Antropomotoryka J Kinesiol Exerc Sci. 2017;25:35-42.
- [Google Scholar]
- Study of the measurement and predictive validity of the functional movement screen. BMJ Open Sport Exerc Med. 2018;4:1-7.
- [CrossRef] [Google Scholar]
- Functional fitness improvements after a worksite-based yoga initiative. J Bodyw Mov Ther. 2010;14:50-4.
- [CrossRef] [Google Scholar]
- Using the functional movement screenTM to evaluate the effectiveness of training. J Strength Cond Res. 2012;26:1620-30.
- [CrossRef] [Google Scholar]
- Functional movement assessments are not associated with risk of injury during military basic training. Mil Med. 2019;184:e773-80.
- [CrossRef] [Google Scholar]
- Functional movement screen normative values in a young, active population. Int J Sports Phys Ther. 2011;6:75-82.
- [Google Scholar]
- Normative data for the functional movement screen in middle aged adults. J Strength Cond Res. 2013;27:458-62.
- [CrossRef] [Google Scholar]




