Translate this page into:
“Effect of Short Term Mild Cold Exposure on Cardiovascular Reflex Responses to Orthostasis by 70 Degree Head-Up-TILT
Abstract
Introduction:
Orthostatic tolerance is reduced in a variety of conditions, like autonomic dysfunction, heat stress, and prolonged bed rest and after actual or simulated microgravity exposure. Substantial benefit would come from the identification of a countermeasure that improves orthostatic intolerance.
Aim:
The purpose of this study was to identify whether short term mild cold air exposure alters orthostatic reactions in otherwise normothermic individuals and explore the possibility of developing cold exposure as a countermeasure against orthostatic intolerance.
Material & methods:
Thermal and cardiovascular reflex responses to orthostatic stress were measured under comfortable ambient temperature (26-28°C) and cold conditions (16°C) in 15 healthy male volunteers, by 70 degree Head Up Tilt(HUT) test on two different days in a cold chamber. On both occasions, after 20 minutes of pre-tilt supine posture, volunteers were exposed to HUT posture for 20 minute. During cold exposure, subjects were exposed to simulated cold environment for 30 minutes which included 10 min of cold exposure in supine posture and 20 minutes in HUT posture.
Results:
Mean skin temperature kept on decreasing throughout HUTT and reduced by 3.5°C over pre-cold exposure value. Oral temperature was not decreased below acceptable limits and none of the subjects felt urge of micturition. There was a significant change in the cardiovascular parameters on assuming orthostatic posture under cold exposure as compared to ambient environmental condition. During HUT Test in cold condition, mean heart rate increased, but to a lesser degree (p<0.001) and greater degree of elevated pressure responses were observed, as compared to normothermic conditions (p<0.001).
Conclusion:
It was concluded that a decrease of mean skin temperature by 2-4°C lead to favourable orthostatic reactions, without causing shivering, presumably via augmentation of Mean Arterial Pressure. Results of the present study suggest a cooling protocol in terms of magnitude, duration and frequency will be beneficial in reduced orthostatic tolerance and cold exposure deserves further exploration as an anti - orthostatic measure.
Keywords
Orthostatic tolerance
Head-Up Tilt test (HUTT)
Mean Arterial Pressure (MAP)
Orthostatic Stress Evaluation Under Cold Exposure

Introduction
Orthostatic intolerance is caused by a variety of conditions, like heat stress, autonomic failure syndromes, prolonged bed rest and after actual and simulated microgravity exposure. Identification of an effective measure against orthostatic intolerance would provide considerable benefit to individuals suffering from above mentioned conditions.
Research has revealed that interventions aimed at increasing blood volume and enhancing vasoconstriction should have the highest likelihood of success as an effective countermeasure [1]. Studies have shown that Skin Surface Cooling (SSC) can provide an alternative method to improve orthostatic tolerance [2-6]. The cooling serves to augment sympathetic activity, constrict skin blood flow, thereby improving central circulation. This would provide restoration of cardiac filling pressure and volume, hence stroke volume. Various authors have reported the beneficial effects of body cooling/skin surface cooling in improving orthostatic intolerance, but optimal temperature, duration and overall protocol still remains debatable. Additional experiments are currently underway which will determine the magnitude, time course, and mechanism of the reflexcardiovascular adjustments that occur with skin cooling.
Previous studies have utilised perfusion of cold water through tube lined suit during lower Body Negative Pressure (LBNP) exposure to show that skin surface cooling, preserves orthostatic tolerance [2-6]. The hypothesis has not been experimentally tested for whole body cooling by cold air exposure, which may also cause favourable cardiovascular reflex responses to orthostatic stress. The purpose of this study was to identify whether short term mild cold air exposure alters orthostatic reactions in otherwise normothermic individuals and explore the possibility of developing cold exposure as a countermeasure against orthostatic intolerance.
Material and Methods
Participants: Fifteen healthy males participated in the study. The participants' mean age was 30 ± 5.4yr, and all were of typical height (174.2 ± 5.58 cm), weight (70.8 ± 5.6 kg), and body surface area of 1.85 ± 0.11 m2. The protocol and informed consent received institutional approval. Written informed consent was obtained from all participants before they enrolled in this study. All subjects were normotensive (supine blood pressures <140/90 mmHg), were not taking medications, and did not have cardiovascular diseases. Subjects refrained from caffeine, alcohol, and exercise 24 h before the study.
Protocol: Cardiovascular reflex responses to orthostatic stress were measured under comfortable ambient temperature (26-28°C) and cold conditions (16°C) in 15 healthy male volunteers, by 70 degree Head UpTilt (HUT) test on two different days in a cold chamber. Subjects were dressed in cotton shorts and vest. On both occasions, after 20 minutes of pre-tilt supine posture, volunteers were exposed to HUT posture for 20 minutes, which was followed by 10 minutes of post-tilt supine posture. During cold exposure, subjects were exposed to simulated cold environment for 30 minutes which included 10 min of cold exposure in supine posture and 20 minutes in HUT posture. Skin temperatures (every 5 min), cardiovascular parameters (every 2 min) and oral temperature (every 5 min) was recorded throughout the protocols.
Measurements: Heart rate and blood pressure were recorded using Agilent M 3046A monitor. Mean Arterial Pressure (MAP) and Pulse Pressure was calculated using standard method. Body temperatures were recorded using a sixteen-channel Intelligent Satellite Unit temperature recorder (Century Systems, Bangalore), which is a micro-controller based multi-channel data acquisition unit. This was used to measure the oral temperature and temperatures from four skin sites i.e. chest, arm, thigh and calf. Mean skin temperature (MST) was measured via the weighted average of four thermocouples attached to the skin.
Statistical analysis: The data were first examined for normality. First 10 minutes data of supine posture has been tabulated in horizontal control category and subsequent 10 minutes under pre-tilt category. For each thermal condition, differences in hemodynamic and temperature variables from supine to HUT posture and comparison between data collected under the two experimental conditions was done using a paired-t test (two tailed dependent).The level of significance was assessed at p<0.05.
RESULTS
Thermal responses: Before cooling and HUT posture, baseline skin (Table-1) and sublingual temperatures were not significantly different between normothermicand cooling protocols, respectively. Cold exposure caused pronounced decrease in MST. After 10 min of cold exposure, just before beginning of HUT, MST was 31.89±0.92°C (p<0.01 vs baseline). MST continued to decrease throughout HUT, resulting in a reduction of approx.3.19°C. MST followed exponential decrease i.e. rate of decrease was higher initially as compared to later part of the experiment. It did not stabilize till the end of the experimental protocol. In post tilt period though MST showed little increase towards the end but values were significantly lower as compared to horizontal control. Under cold exposure oral temperature did not decrease more than 0.5°C for any of the subjects. None of the subject reported shivering.
| Variable | Baseline (first 10 min, horizontal control) | Cold exposure (next 10 min, end of pre-tilt) | End of HUT |
|---|---|---|---|
| Mean skin Temp °C | |||
| Normotherm | 33.49±0.79 | - | 33.47±0.86 |
| Cooling | 33.55±0.77 | 31.89±0.92** | 29.97±0.95** |
| Oral temp °C | |||
| Normothermia | 36.5±0.36 | - | 36.5±0.39 |
| Cooling | 36.39±0.62 | 36.27±0.64 | 36.l±0.61 |
All values are mean ± SD. ** Significant for the event (p value: p ≤ 0.01) from base line
Responses to HUTT : The effects of cold exposure on hemodynamic variables are reported in Table 2.
| Cardiovascular Parameters | Pre Tilt | HUT(0-10 min) | HUT(12-20 min) | Post Tilt |
|---|---|---|---|---|
| Ambient Temperature | ||||
| HR (bpm) | 72.36 ±7.80 | 83.33 ± 7.06** | 82.95 ± 8.86** | 72.40 ± 7.98 |
| SBP (mm Hg) | 115.08 ±5.97 | 114.11 ±5.71 | 113.65 ±8.17 | 114.4 ±6.38 |
| DBP (mm Hg) | 71.98 ±6.33 | 79.28 ± 6.43** | 78.33 ± 6.29** | 72.49 ± 6.24 |
| MAP (mm Hg) | 86.30 ± 5.62 | 90.86 ±5.71** | 90.12 ±5.81** | 86.6 ± 5.55 |
| PP (mm Hg) | 43.10 ±5.55 | 34.83 ± 5.25** | 35.32 ±4.77** | 42.32 ± 5.24 |
| Cold Temperature | ||||
| HR (bpm) | 69.86 ±7.35 | 76.02 ± 6.99**## | 75.28 ± 7.05**## | 69.99 ± 6.73 |
| SBP (mm Hg) | 118.11 ±5.61 | 122.86 ±5.99**## | 123.16 ±8.17**## | 119.33 ±5.12 |
| DBP (mm Hg) | 74.59 ± 6.29 | 86.23 ± 5.47**## | 86.18 ±5.61**## | 77.88 ± 5.70* |
| MAP (mm Hg) | 89.09 ± 5.44 | 98.13 ±5.01**## | 98.56 ± 5.20**## | 91.89 ±4.91* |
| PP (mm Hg) | 43.50 ±5.66 | 37.52 ± 6.07**## | 36.97± 5.25**# | 41.96 ±4.69 |
Under ambient temp during HUTT the mean Heart Rate (HR) attained during first 10 minutes (83.33 ± 7.06 bpm) and subsequent 10 minutes (82.95 ± 8.86bpm) was significantly higher (p<0.001) than corresponding values (76.02 ± 6.99 and 75.28 ± 7.05 bpm) under cold stress. Mean change of 5.83 ± 1.99 bpm under cold exposure was significantly lower than mean change of 10.8 ± 2.92 in ambient temperature (Fig-2).

- Mean skin temp (°C) response under cold condition (Values are expressed in mean ± SD)
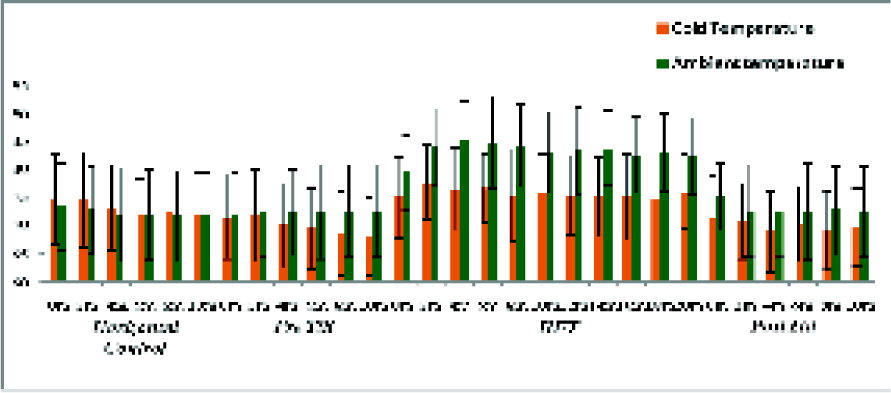
- Heart Rate (bpm) responses under ambient and cold condition (N=15) (All values are in mean±SD. For statistical significance refer text.)
Under ambient temp mean Systolic Blood Pressure (SBP) attained during first 10 minutes of HUTT (114.11 ± 5.71mmHg) and subsequent 10 minutes of HUTT (113.65 ± 8.17 mmHg) was significantly lower (p<0.001) than corresponding values of SBP attained (122.86 ± 5.99 andl23.16 ± 8.17 mm Hg) under cold exposure (Fig-3).
- Comparison of Mean Change in Systolic BP (mm Hg) between pre-tilt and tilted posture for ambient and cold condition (N= 15)
During HUTT mean change of 4.88 ± 1.96 mmHg, observed under cold exposure was significantly higher than -1.17 ± 0.99 mmHg under ambient condition (p<0.001).
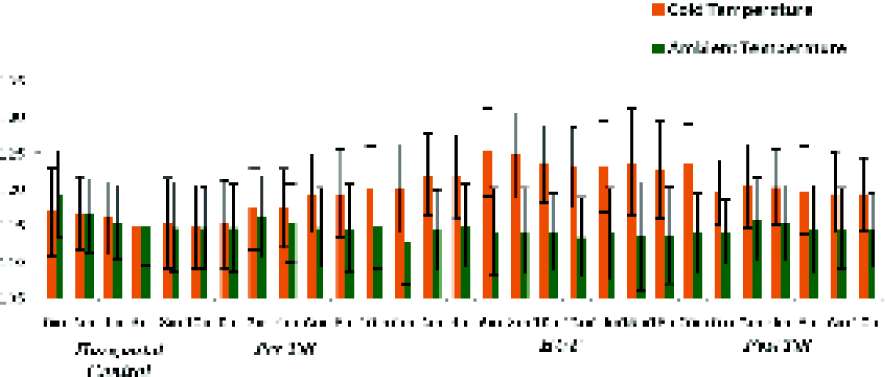
Under ambient temp, during HUTT, the mean Diastolic Blood Pressure (DBP) attained during first 10 minutes (79.28 ± 6.43mmHg) and subsequent 10 minutes (78.33 ± 6.29 mmHg) was significantly lower (p<0.001)than corresponding values (86.23 ± 5.47 and 86.18 ± 5.61mmHg) under cold exposure (Fig-4).
- Diastolic BP (mm Hg) response under Ambient and cold condition (All values are in mean±SD. For statistical significance refer text)
During HUTT mean change of 11.62 ± 2.58 mmHg, observed under cold exposure was significantly higher than 6.87 ± 0.72 mmHg under ambient condition (p<0.001).
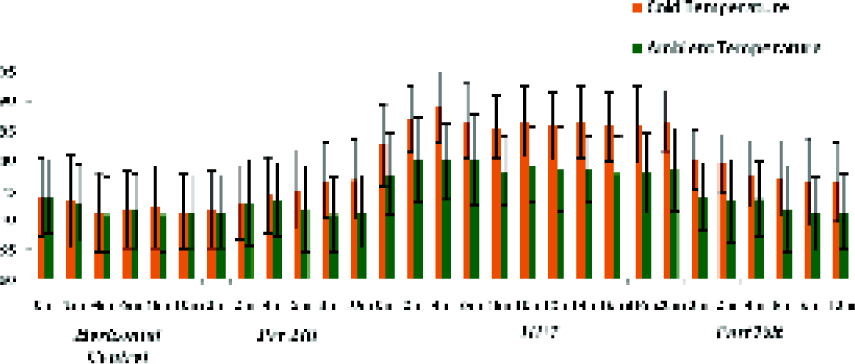
Under ambient temp during HUTT the mean MAP attained during first 10 minutes (98.13 ± 5.01mmHg) and subsequent 10 minutes (90.12 ± 5.81 mmHg) was significantly lower (p<0.001)than corresponding values (98.13 ± 5.01and 98.56 ± 5.20mmHg) under cold stress (Fig-5).

- Mean Arterial Pressure (mm Hg) response under ambient and cold condition
- (All values are in mean±SD. For statistical significance refer text)
During HUTT mean change of 9.24 ± 1.78 mmHg, observed under cold exposure was significantly higher than 4.22 ± 0.51 mmHg under ambient condition (p<0.001).
DISCUSSION
Previous reports suggested that skin surface cooling (SSC) improves orthostatic tolerance in normothermic and heat stressed subjects [2-6]. Most of these studies utilised perfusion of cold water through tube lined suit and LBNP exposure to demonstrate the effect of skin surface cooling on orthostatic hemodynamic responses. In the present study, an attempt was made to investigate whether short term mild cold air exposure also causes favorable hemodynamic responses to orthostasis.
Under cold exposure, a reduction of 3.59 ± 0.34°C in MST was observed over horizontal control value at the end of 20 minutes of HUTT. During the total duration of cold exposure (30 minutes), MST did not stabilise and kept on decreasing, though the rate of fall was lower during last 10 minutes as compared to first 10 minutes of cold exposure. Makinen TM et al, investigated autonomic nervous function during whole body cold exposure before and after cold acclimation by exposing 10 young males to 10°C for 2 hours daily in cold chamber for 20 days. On first day, during first hour, a decrease in MST by 6.5°C was reported [7]. DIPAS in 1990 conducted study on artificial cold acclimatization by exposing 15 young men to 10°C for 4 hours daily in cold chamber for 20 days. On the first day, during first hour, a decrease in MST by 6°C was reported, which stabilized thereafter [8]. Higher fall in MST in these studies was reported, probably because of lower cold air temperatures used. In post-tilt period MST reverted back to pre-tilt value, but remained significantly lower as compared to horizontal control, sustaining CVS response for longer time. Oral temperature did not decrease below acceptable limits no shivering was reported and no urge for micturition occurred in any of the subjects, indicating the tolerable degree of cold stress.
Under cold exposure the increase in HR during orthostatic stress was significantly lower as compared to ambient temperature, which corroborate with the findings of other researchers in this field. In both experimental conditions, mean HR during first 10 min of tilt did not show significant difference from subsequent 10 minutes which indicates that increase in HR was sustained throughout 20 min of tilt. Wilson T E et al, Durand S, Raven P B et al, reported attenuation in HR during tilt under cold exposure as compared to normothermic subjects [2,3,5]. The reasons cited in these studies are, that increased Total Peripheral Resistance due to vasoconstriction in conjunction with augmented pressure responses and Central Venous Pressure (CVP) works as a depressor of heart rate and this probably explains why the heart failed to respond to increased circulatory demand. Cold air exposure to face also initiates a vagal response due to stimulation of Trigeminal Nerve of the face leading to bradycardia [9].
During HUTT, as compared to ambient temperature, mean SBP under cold exposure showed significantly higher value (113.90 ± 5.52 vs. 122.99 ± 5.87mmHg) (p<0.001). A difference of 9.09 ± 3 mm Hg was observed. Raven et al investigated compensatory cardiovascular responses during an environmental cold stress of 5°C. The results of the study demonstrated a rise in SBP due to shift of peripheral blood volume into the central circulation, eventually leading to increase in stroke volume (SV) and cardiac output (CO) [9]. Similar findings under cold air exposure at different temperatures have been reported by Makinen TM et al and DIPAS [8]. Data of present study suggests greater cutaneous and peripheral vasoconstriction causing a larger shift of peripheral blood volume into the central circulation during orthostasis, improving venous return, SV and thus SBP.
In contrast to SBP, DBP values were significantly higher (p<0.001) during HUTT in both experimental conditions over pre-tilt value. Hence a greater degree of increase in DBP was seen under cold exposure as compared to ambient temperature, which is statistically significant (p<0.001). Wilson TE et al and Cui J et al also reported significant increase in DBP due to rise in TPR [2]. Durand S et al reported substantial increase in DBP due to increased plasma Norepinephrine concentrations during LBNP with SSC [3]. Our data on HUTT under cold condition probably suggests greater sympathetic activation and peripheral vasoconstriction as compared to ambient condition leading to higher values of DBP.
During HUT posture under cold condition a significant increase (p<0.001) in MAP of 9.24 ± 1.78 mmHg was observed over pre-tilt value, which is significantly higher than rise of 4.22 ± 0.51mm Hg in ambient temperature. Above mentioned studies reported higher degree of rise in MAP (by approx. 1315mm Hg) during orthostatic stress over baseline value as compared to the present study (by approx.9-llmm Hg). This may be due to higher rates of skin cooling achieved by perfusion of cold water as mentioned above. Makinen and Raven also reported higher sympathetic activation and increased plasma Norepinephrine levels for significant rise in MAP under cold air exposure [7,9].
Adequate arterial blood pressure is the key component in the maintenance of cerebral blood flow and the orthostatic tolerance. Prior to HUT posture, cold exposure increased MAP by approx. 4 mm Hg, and blood pressure remained significantly elevated throughout HUT posture. Arterial blood pressure is the product of cardiac output and vascular resistance. As SV, CO and vascular resistance were not measured in the present study, it is not clear, whether the elevation in arterial blood pressure during tilt under cold exposure was due to elevated cardiac output and/or elevated vascular resistance. Increase in HR during tilt under cold exposure, coupled with elevated blood pressure; probably suggest that cardiac baroreflexes were reset as a result of cooling. Therefore, prior to HUT posture the baroreflex resetting and perhaps increase in peripheral resistance are likely the main factors responsible for the elevation in arterial blood pressure during cooling. During HUTT under cold exposure, increased pressure responses are likely to be related to greater sympathetic activation, increased peripheral resistance, increased cardiac filling pressure leading to increased SV and CO. It can be speculated that orthostatic stress and cold exposure is likely to produce synergistic effect to alter cardiovascular reflex responses in a beneficial way.
Favourable cardiovascular responses were observed in post-tilt period also as compared to horizontal control values, indicating that decreased MST may have prolonged the effects of cold exposure on CVS parameters.
Conclusion
Together these observations suggest that the effects of mild cold exposure on augmenting pressure responses may contribute to an improvement in orthostatic tolerance. A decrease of approx. 3 °C in MST appeared sufficient in improving orthostatic reactions in normothermic individuals. Regardless of the mechanism, these data demonstrate that cold exposure may be an effective countermeasure against reduced tolerance known to occur in Autonomic Insufficiency Syndromes, after prolonged bed rest and space flight. There is a possibility that mild cold air exposure can be developed as an anti-orthostatic measure. To explore this possibility further experiments are required with larger sample size, under different simulated conditions (simulated microgravity) and on individuals suffering from OI.
Disclaimer
The opinions expressed in this article are those of the author do not reflect the official views of the Indian Air Force.
Or the Indian Society of Aerospace Medicine
References
- Post flight orthostatic intolerance. In: Space Physiology (1st ed). New York: Oxford University press; 2006. p. :153.
- [Google Scholar]
- Skin cooling maintains cerebral blood flow velocity and orthostatic tolerance during tilting in heated humans. J. Appl. Physiol. 2002;93(1):85-91.
- [Google Scholar]
- Skin surface cooling improves orthostatic tolerance. Am J Physiol Regulatory Integrative Comp Physiol. 2004;286(1):199-205.
- [Google Scholar]
- Effect of Skin surface cooling on CVP during an orthostatic challenge. American Physiological Society.
- [Google Scholar]
- Hemodynamic changes during whole body surface cooling and lower body negative pressure. Aviation Space Environ Med. 1981;52(7):387-91.
- [Google Scholar]
- Interactions between surface cooling and LBNP-induced central hypovolemia. AviatSpace Environ Med. 1980;51(5):497-503.
- [Google Scholar]
- Autonomic nervous function during whole-body cold exposure before and after cold acclimation. Aviat Space Environ Med. 2008;79:875-82.
- [Google Scholar]
- Physiological adaptation to severe cold In: Selvamurthy W, Sridharan K, Chandhu BN, eds. Stress physiology. New Delhi: DRDO; 1989. p. :98-105.
- [Google Scholar]
- Compensatory cardiovascular responses during an environmental, cold stress,5°C. J ApplPhysiol. 1970;29:417-21.
- [Google Scholar]




