
Translate this page into:
C130J: IAF’s Hercules in casualty/medical evacuation

*Corresponding author: Mohin M. Sakre, AFS Arjan Singh, Panagarh, West Bengal, India. drmoinsakre@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Sakre MM, Jhamb D, Dutt M, Mukul SD. C130J: IAF’s Hercules in casualty/medical evacuation. Indian J Aerosp Med 2023;67:46-53. doi: 10.25259/IJASM_19_2023
Abstract
Objectives:
This study looks to evaluate the casualty/medical evacuation capabilities of the Indian Air Force’s formidable C130J-30 in terms of patient carrying capacity patient support facility while also assessing its aeromedical issues.
Material and Methods:
This descriptive report employs a detailed and analytical evaluation of an on-ground parked C130J-30 Super Hercules. In addition, manuals have been referred to; data have been inferred from real-life experiences, and drills and inputs from the aircrew through interview methods have been incorporated.
Results:
The C130J has a seated casualty carrying capacity of 98 and a lying casualty carrying capacity of 97 patients, and lying casualties require the employment of specifically designed litters (stretchers). Medevac requires the use of a specially and specifically designed patient transport unit with a cumulative battery life of around 3.5 hours. The cargo compartment has Four 300 Psi cylinders and 30 LOX O2 systems for emergency use. Available ports in the cargo compartment supply 115 V AC 3 phase 400 Hz. The vibration profile of the aircraft ranges up to 85–100 Hz, and cargo compartment noise levels range between 80 Hz and 118 Hz.
Conclusion:
This paper satisfactorily concludes that the C130J is undoubtedly an unmatched asset in the casualty/medical evacuation capabilities of the Indian Air Force.
Keywords
Casualty evacuation
Medical evacuation
Casevac/medevac
Indian Air Force
C130
May C17 Globemaster

INTRODUCTION
The Lockheed Martin C130J-30 Super Hercules has been affirmatively Herculean in its assigned tactical capabilities of being a Special Ops Multi-Role Transport Aircraft. Drafted in the compellingly robust arsenal of the Indian Air Force (IAF) in 2010–2011, the upgraded and modified version of the US beast has a wing span of 132 feet 7 inches, a length of 112 feet 9 inches, and maximum cruise speed of 355 Kts running on Four Propeller based Rolls Royce AE2100 D3 engine.[1]
The historically stoic aircraft has been a pioneer in its Casevac/Medevac capabilities since 1970, when it was first used to transport Red Cross hospital equipment and patients in Kitzingen Airbase, Germany. Subsequently, the aircraft has demonstrated its mettle in war evacuation in Vietnam, earthquake relief in Haiti, and Medevac in Bagram, Afghanistan, to enumerate a few.[2] In recent times in India, the C130J Hercules has been monumental in its efforts in COVID containment and prevention, emergency Casevac missions, and, when equipped with its specially and specifically designed patient transport unit (PTU), as a formidable Medevac contrivance.[3]
Objectives
This study looks to evaluate the casualty/medical evacuation capabilities of the C130J-30 in terms of patient carrying capacity and patient support facility while also assessing its Aeromedical Issues. An attempt has also been made to draw certain comparisons with its counterpart, the other American Aircraft used by the IAF in Cas/Medevac: Pratt and Whitney Jet engine-based Boeing Globemaster C17. The objective is to assess and establish capabilities, convenience, and ascendancy in employability for casualty/medical evacuation of one over the other.
MATERIAL AND METHODS
This descriptive report employs a detailed and analytical evaluation of an on-ground Parked C130J-30 Super Hercules aircraft in one of the most cardinally paramount Air Force Stations of the Eastern Air Command, IAF.
The following methodology was arrogated when various aspects of the aircraft were probed and scrutinized:
Aircraft manuals available on open source internet[4]
Physical Exploration of the Aircraft
Interactions with the aircrew
Experiences drawn from drills and previously conducted Casevac and Medevac.
Certain aspects of contemporary aircraft, namely, the C17, were also compared in the scope of this study through physical exploration of the aircraft and interactions with the crew of the C17.
RESULTS
The aircraft usually employs a crew of four (Pilot, Co-pilot, Combat Systems Operator, and Load Master) for cargo operations. It can reach a service ceiling of 28,000 feet comfortably and has an absolute ceiling of 32,000 feet.[5] It has an unrefueled endurance of approximately 12 hours. It can burden a maximum alternate take-off weight of around 175,000 lbs. The cargo compartment’s dimensions are 56 feet in length, 10 feet 3 inches in width, and 9 feet in height. Its special operational capabilities are demonstrated by its capacity to operate from runways as short as 3000 feet and as narrow as 50 feet made of just dirt and no tarmac.[6,7] The passenger/cargo compartment is well-lit and equipped with anti-skid flooring.
The large volume of the cargo compartment of the C130J-13 is the primary benchmark of the aircraft that makes it desirable for casevac, however, it is not the only criterion that makes it so apt for the said role. The C130J-30 can carry max 128 seated passengers/patients (including the seats for med asst and 02 Load Masters). The C17 has a seated casualty carrying capacity of 90 persons.[8]
Evacuation of lying casualties necessitates the use of stretchers. While in Med evacuation, a single stretcher mobile with roller wheels can be hooked onto the floor of the Aircraft, mass casualty evacuation requires the employment of stanchions. One stanchion can accommodate 4 L at the side wall and 5 L (stretchers) stations at maximum (with a vertical space of 18 inches between each litter) in the center. This set-up of the vertical stanchion and the attachable 04/05 L fabricates the aeromedical station of the Hercules. The dimensions of the litter are 7.5 × 2 feet with a handle circumference of 4.5 inches. Scoop stretchers or hospital foldable stretchers are not compatible with the hook bracket of the stanchion.
The stanchion has a free-standing design and is stowed onboard the aircraft, ensuring the aircraft is launch-ready in short durations. The necessary modification for mass Casevac may be done en route after loading the mandatory litter. This modification caters to 97 lying casualties en-masse [Figure 1].[7] The C17 has the maximum carrying capacity of only 36 lying casualties. A patient in PTU requires the area of one whole stanchion, that is, 28 sq. ft (One person on the ventilator as opposed to four to five who are not). The loading-unloading technique of first in-first out and “Z” pattern of casualty allotment of litter is adopted post-triage on the basis of severity and benefit of the intervention.

- Stanchion and attached stretchers (Source: Open-source internet).
Various combinations of aeromedical evacuation are also possible:[8]
Aeromedical evacuation (AE) 1 [Figure 2]: 30 L + 60 seats
Aeromedical evacuation (AE) 2 [Figure 3]: 97 L
Aeromedical evacuation (AE) 3 [Figure 4]: 20 L + 60 seats
Aeromedical evacuation (AE) 4 [Figure 5]: 60 L + 60 seats.
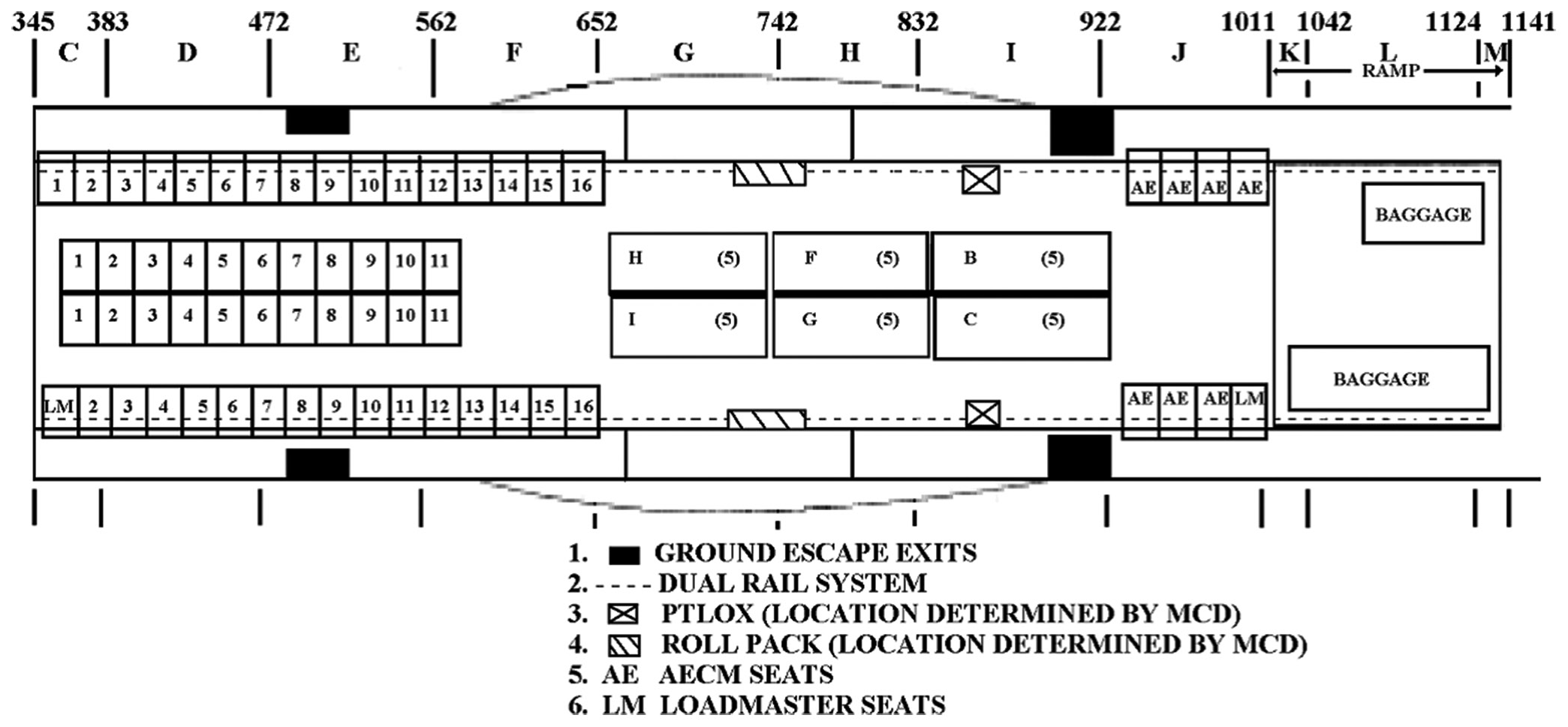
- AE 1 (Source: Open-source internet), MCD: Main Cabin Door, AE: Aeromedical Evacuation, AECM: Aeromedical Evacuation Crew Members, LM: Loadmaster.
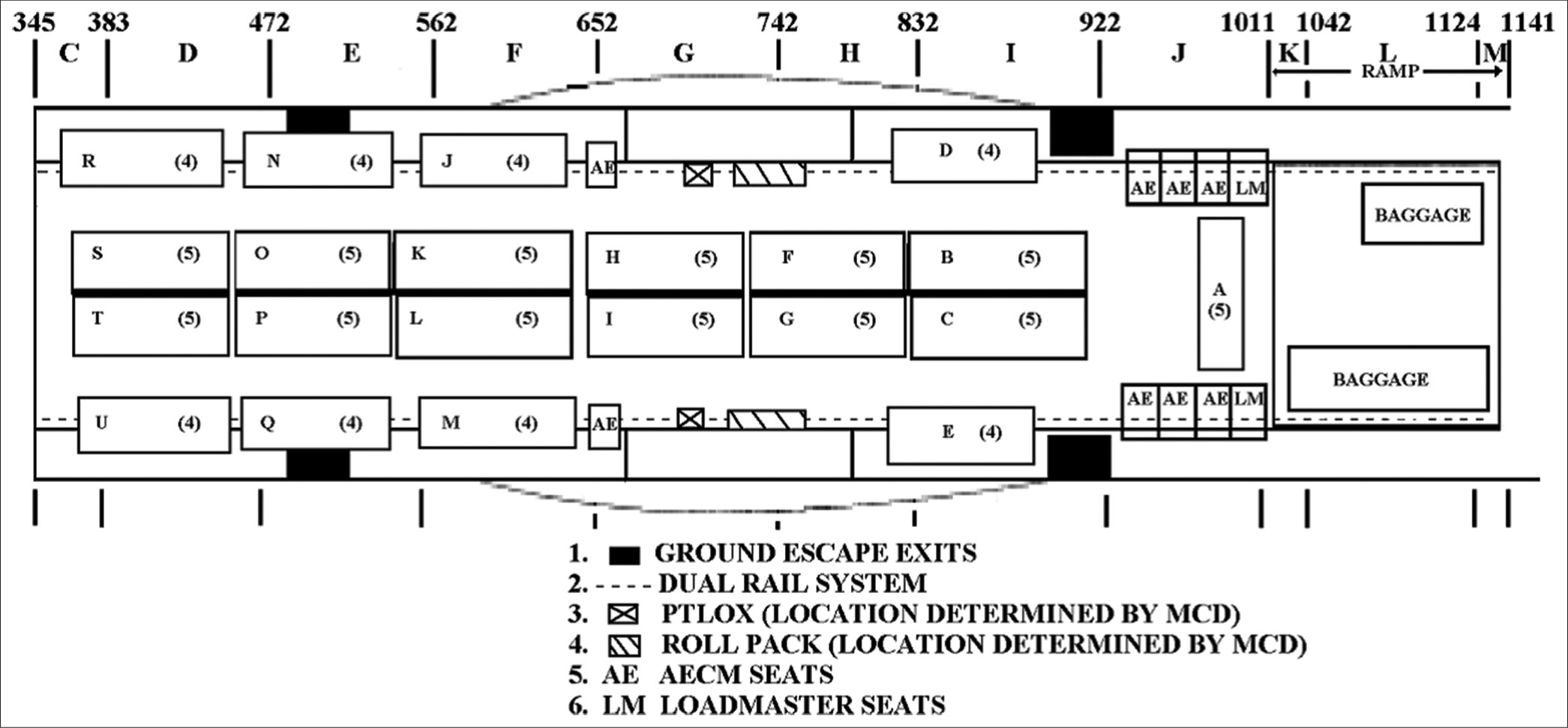
- AE 2 (Source: Open-source internet). MCD: Main cabin door, AE: Aeromedical evacuation, AECM: Aeromedical evacuation crew members, LM: Loadmaster.
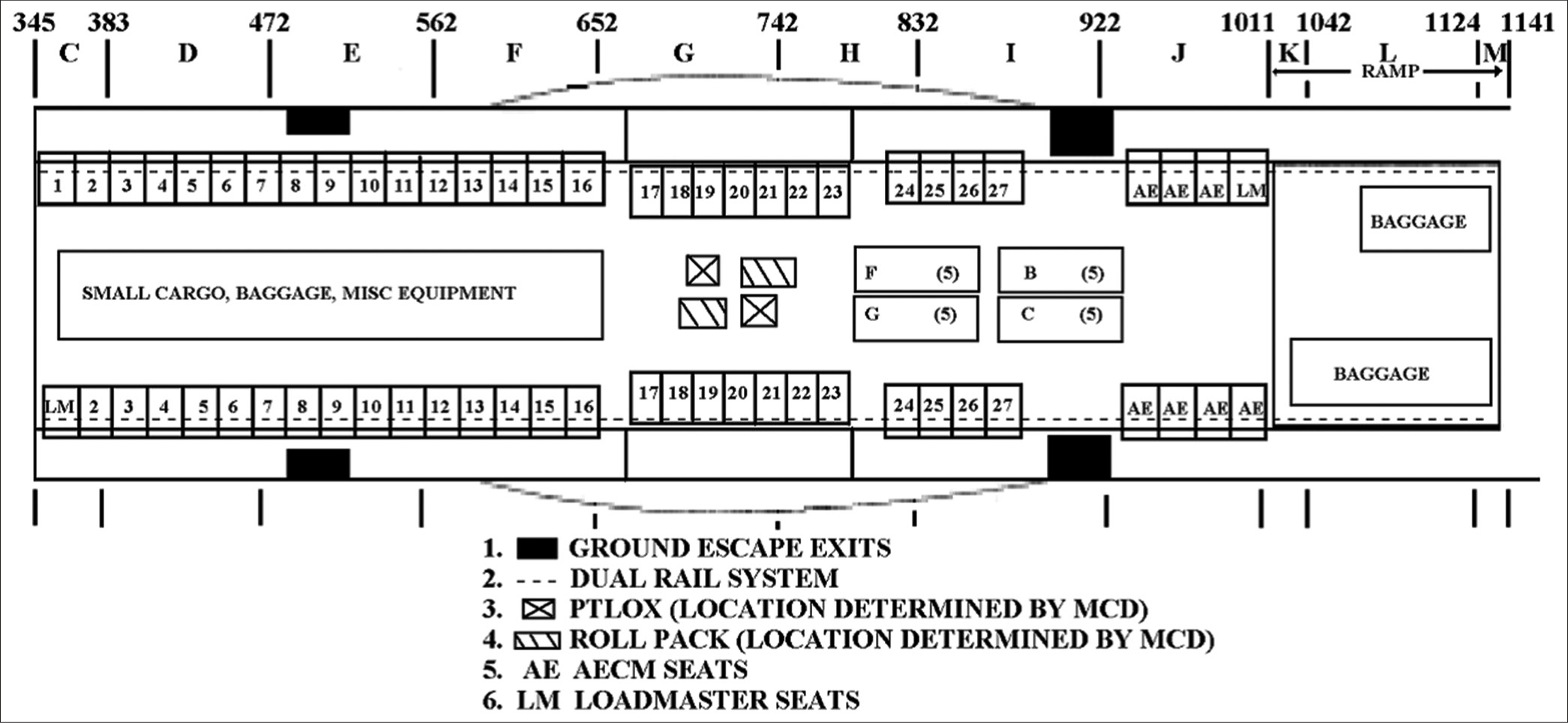
- AE 3 (Source: Open-source internet). MCD: Main Cabin Door, AE: Aeromedical Evacuation, AECM: Aeromedical Evacuation Crew Members, LM: Loadmaster.
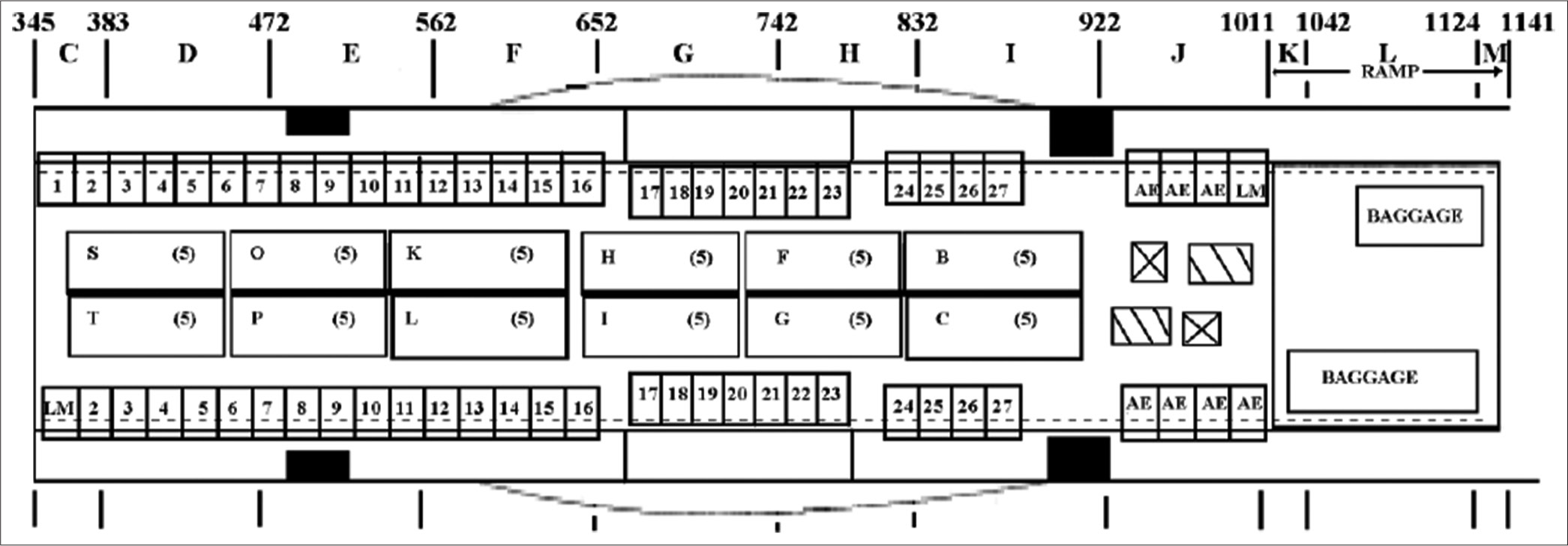
- AE 4 (Source: Open-source internet). MCD: Main cabin door, AE: Aeromedical evacuation, AECM: Aeromedical evacuation crew members, LM: Loadmaster.
Besides these, any combination can be adopted based on requirements and operational demands.
All the above combinations account for the presence of two load masters and five medical representatives at the least. All seated patients are safely secured in their places with a harness. In case of an infelicitous incident en route, each seated passenger is provided with an emergency passenger oxygen system (EPOS), which is an oxygen mask that is a lightweight, self-contained protective breathing device or a smoke hood for use in emergency egress and escape situations [Figure 6].
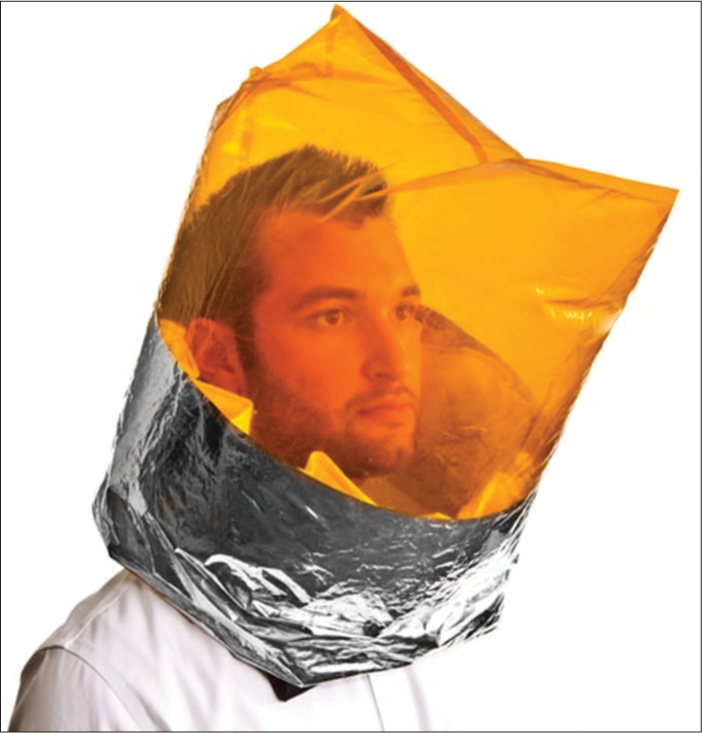
- Emergency Passenger Oxygen System (Source: Open Source Internet).
Patient care and support in Cas/Med evacuation on the C130-J-30 is provided by a specially and specifically assorted PTU [Figure 7] complete with the following:
Ventilator
Multi para monitor
Defibrillator
Infusion pump
Suction
Oxygen cylinders (1248 L).

- Patient transport unit
In addition, any required battery-run medical equipment can be added to the PTU. The tried average battery life of the amalgamation of the above medical equipment is around 3–3.5 hours. This can suffice for almost all the routes across the length of the country. Superimposing the three-and-a-half-hour life of the consorted PTU, lead-free lithium-ion batteries having 2 KVA output at 28 V DC batteries with 40 Ah can also be utilized to charge and enhance the endurance of the electromedical equipment with a backup of 4–4.5 hours. The medical workforce designated to operate the aeromedical setup on board the aircraft needs to be implicitly trained to operate the equipment, thereby ensuring patient safety.
A brief comparison of some of the important criteria that are critical for Casevac/Medevac [Table 1] has been tabulated below:
| Criteria | C130J-30 | C17 |
|---|---|---|
| Make | Lockheed Martin (US) | Boeing (US) |
| Engine | Propellor (Rolls Royce) | Jet (Pratt and Whitney) |
| Top speed | 590 km/h | 950 km/h |
| Min length of runway required for take-off | 3000 feet | 3500 feet |
| Service ceiling | 35000 feet | 45000 feet |
| Maximum take-off weight | 155000 lbs | 170900 lbs |
| Cargo compartment dimensions | ||
| Length | 41 feet (12.5 m) | 88 feet (27 m) |
| Width | 10 feet (3.05 m) | 18 feet (5.5 m) |
| Height | 9 feet (2.74 m) | 12.4 feet (3.76 m) |
| Casualty carrying capacities | ||
| Seated | 128 | 90 |
| Lying | 97 | 36-40 (with ramp loading) |
| Accommodating a PTU | 01 PTU potentially takes up the space of 04-05 L (stretchers) |
01 PTU potentially takes up the space of 03 L (stretchers) |
| Best possible combination | 60 lying + 60 seated casualties | 24 lying + 36 seated casualties |
| Support for EM equipment and patient support | ||
| Life support augmentation system: To stow O2 and EM eqpt | Absent | Present |
| static frequency convertor: To charge EM eqpt | Absent | Present |
| O2 for patients | In-built LOX: Present but not designated for patients per se |
36 L of In-built LOX designated specifically for patients |
EM: Electromedical, PTU: Patient transport unit, LOX: Liquid oxygen.
Irrespective of the type of aircraft used for Casevac/Medevac, it is imperative that the medical agency caters to the patients’ emergent and critical medical requirements. Exceeding the equipment available onboard the aircraft for med support, C130s quick launch capability ensures the timely scoop and scoot in mass casualty evacuation or meticulous medical evacuation. Additional to the oxygen loaded with the PTU, the cargo compartment of the Hercules has two in-built O2 systems and four portable O2 cylinders of 300 PSI each [Figure 8] that last from 10 min to 1 hour primarily installed for the aircrew. The built in oxygen systems draw oxygen from the centrally installed 36 LOX O2 container. In dire situations, these sources of oxygen can also be used as a life-saving measure.

- Portable O2 (300 Psi cylinder) (Source: Open source internet).
In regards to the electrical system of the aircraft, a provision exists of supply of 115 V AC and 28 V DC current. Available ports in the cargo compartment supply 115 V AC 3 phase 400 Hz.[4] On facilitating a convertor to 230 V single phase 50 Hz, this supply can be used to power the electromedical equipment used in medical evacuation. This mechanism is in use on the C17 and may be attempted to be instrumented on the C130-J-30 on obtaining astute air worthiness. Both the aircrafts have American style “Type A and B” power plugs and sockets which mandate the use of any standard conversion plug of “Type B, C and D.”[9]
Patient comfort and ambient environment are ensured by the adept pressure and temperature control of the aircraft. Hercules is equipped with a state-of-the-art pressurization control panel capable of maintaining a wide range of cabin altitude from sea level to 9000 feet. The C130J has a Constant Altitude Mode, which enables the crew to control the cabin pressure at a comfortable 4000 feet, even at actual heights of >9000.[10] The aircraft is equipped with two separate air conditioning systems, one for the cargo compartment and another for the flight station, complete with a compartment temperature sensor and a duct overheat sensor, maintaining the cargo compartment temperature at comfortable levels.[11] The vibration profile of the aircraft ranges up to 85–100 Hz[12], and cargo compartment noise levels range between 80 Hz and 118 Hz.[13] The lighting in the cargo compartment of the C130 is sufficiently well-lit to cater for interventions on board if required. It is also augmented with the Infrared lights in the Cargo Compartment, further substantiating its Casevac role even in combat capabilities.
DISCUSSION
The Lockheed Martin’s modified C130-J-30 has been effective in its special-ops role in the IAF since its commissioning in 2010–2011. Its tactical and operational role has been illustrated in several challenging missions such as low-altitude load drops, long haul sorties, low-level flight at a meager 400 feet, impeccable maneuverability, and ease of transgression in difficult flight paths, including night sorties. From a medical perspective, the aircraft has been prodigious in Casevac and guileless in its medevac capabilities. The aircraft has NVG capability aid of its EOR Cameras, thereby making it conducive for Night time Casevac and Medevac operations as well, especially in Combat Scenarios.
Its’ seated patient carrying capacity of 128 makes it the largest aircraft used in Casevac among the plethora of commissioned IAF airships. The design and the convenient size of the cargo compartment enable it to seat more than its larger American counterpart C17.[9] Physical exploration of both aircraft has revealed that the reason for this could be the enormous size of the cargo compartment of C17. The large airframe on the Boeing counterpart of the super Hercules makes the seating of casualties in the center undesirable due to the lack of support in the form of back rest and harness attaching hooks.
Even in the litter embedding stanchion mode required for lying casualties, the C130 is capable of accommodating more casualties than the C17 due to accessibility to the roof of the aircraft. The large size of the C17 renders the ceiling of the cargo compartment inaccessible, due to which specially designed self-supporting stanchions are fabricated which are installed on the floor of the aircraft and are supported through a horizontally angled iron frame between the two vertical frames of the stanchion system [Figure 9]. The stanchions on the C130 are supported from the floor as well as the ceiling of the cargo compartment [Figure 1]. This provides sturdier support to the stanchion system, thereby enabling accommodation of up to five casualties as opposed to the maximum of three on the C17. In both aircraft, the litters are detachable from the stanchion and facilitate need-based manipulation such as 2 L per stanchion and even floor loading of the litter. Various pre-determined and practiced combinations of seated and lying casualties ensure op-readiness and quick despatch at all times.

- The stanchion system on the C17 without any support from the ceiling (Source: Open source internet).
Seated ambulatory patient, passenger and aircrew safety is ensured by measures such as EPOS [Figure 6], portable O2 cylinders [Figure 8], and built in LOX systems. Medical evacuation on board the C130 is tenable through a consortium of electromedical equipment comprising a ventilator, multipara monitor, defibrillator, infusion pump, suction pump, and aluminium oxygen cylinders mounted on a mobile stretcher that encompasses two aluminium 1248L O2 cylinders. This consortium with a battery life of around 4–4.5 hours is sufficient to cater to medevac missions across the length and breadth of the country. This consortium of equipment that makes up the PTU [Figure 7] of the C130 is rolled on a rollable and foldable stretcher. The wheels are foldable to half their height (For to Two feet) and the stretcher with all its appendages can be latched on to the floor of the cargo compartment using the provided restraints and hooks on the floor of the cargo compartment.
While the aeromedical stations are stowed in a cabinet on the C17 in the form of a life support augmentation system, the provision of a PTU with a Power Backup Unit makes the C130 at par with the C17 in its medevac capabilities. However, procurement of C130J compatible medevac setups such as those in use in the USAF (Knight Aerospace medical module, etc.) may also be considered.[14] The specially designed Medical Evacuation models are custom-made to the needs of the aircraft, such as compatible electrical input systems, and can vary from loadable stretchers with attached medical equipment to a specifically designed aeromedical biocontainment system, immediately available as mobile emergency rooms. Twelve such mobile rooms can be accommodated in the cargo compartment of the C130J. The financial implications of such models are not standardized and vary depending on the needs of the purchasing organization.[14]
The 115V 3 phase 400 Hz electrical supply[7] on the aircraft is not compatible with the electromedical equipment of the PTU. The C17 also has the same electrical output but utilizes a static frequency converter to harvest a 230 V single-phase 50 Hz supply. While the existing medevac setup of a PTU with a PBU is effective with a total power output of around 4–4.5 h, contemplating the installation of a convertor on the C130 to enable en-route charging of the electrical equipment may aid in enhancing the op-readiness of the aircraft.
Patient comfort on board is ensured by dint of “constant altitude pressurization control” mode that ensures cabin pressure of 4000 feet even at heights above 9000.[10] The separate air conditioning system of the cargo compartment with duct overheat sensor and compartment temperature sensor[11] ensures an ambient environment and isolation of ventilation source for the aircrew and the patients. Regarding patient discomfort as a result of the vibration profile of the cargo compartment of the C130J, an Australian study conducted to assess the effects of vibration on board the Hercules concluded that the vibration levels on the C130-J-30 are highly unlikely to pose any short-term or long-term deleterious effects.[12] The noise level in the cargo compartment of the C130J-30 can reach up to a maximum of 118 Hz[13], while that in the C17 can reach around 90 db.[9] Prioritizing agility, ease, covert capability, patient carrying capacity, medevac proficiency, and convenience of Cas/Medevac on the C130 and considering the fact that the exposure is only for a short duration of time, the slightly higher noise levels in the cargo compartment of C130 as compared to C17 can definitely not be considered a disadvantage. However, silicon/foam/cotton earplugs may be used to mitigate the discomfort.
CONCLUSION
Lockheed Martin C130-J-30 Super Hercules is an efficacious aircraft in its various assigned special ops roles. A pioneer in casualty evacuation, its capabilities in the said arena include short time of operational readiness, long haul evacuations, the potential of operating in arduous and testing conditions, the capacity of mass casualty evacuation, facilitation of specialized intervention with the aid of specifically designed PTU, covertness, low level (altitude) flying capability, ample patient support facility, and provision of a comfortable ambient environment. To further enhance the productiveness and op readiness of the aircraft, the following enhancements can be made:
A static frequency convertor may be employed to convert the 115V 3 phase 400 Hz electrical supply which cannot be used to charge electromedical equipment onboard the aircraft, to a 230 V single phase 50 Hz supply.
Procurement of C130J compatible medevac setups, such as those in use in the USAF (Knight Aerospace medical module, etc.), may also be considered.
Ethical approval
The research/study complied with the Helsinki Declaration of 1964.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Steady and ready: C-130 Mainstray of medevac. Available from: https://www.airforcemedicine.af.mil/Platforms/Steady-and-ready-C-130-mainstay-ofmedevac [Last accessed on 2022 Jun 11]
- [Google Scholar]
- A quick look at why the C130 is still USAF Mainstray of Medevac more than 60 years after its first flight USA: The Aviation Geek Club; 2018.
- [Google Scholar]
- Lockheed Martin. 2019. Hercules history. United States: Lockheed Martin; Available from: https://www.lockheedmartin.com/en-us/products/c130/history.html [Last accessed on 2019 Apr 06]
- [Google Scholar]
- Flying operations: C-130J operations procedures In: Air force manual: 11-2C-130J. Vol 3. United States: USAF; 2021.
- [Google Scholar]
- Dirt qualified: Maximum effort landings in the C-130. 2015. SOFREP-Military Grade Content. Available from: https://sofrep.com/fightersweep/maximum-effort-landings-inthe-c-130 [Last accessed on 2022 Jun 11]
- [Google Scholar]
- Flying operations: C-130J operations procedures In: Air force manual: 11-2C-130J. Vol 3. United States: USAF; 2021.
- [Google Scholar]
- C130J operations configuration/mission planning In: Airforce instructions 11-2C-130J. Vol 3. Washington, DC: USAF; 2009.
- [Google Scholar]
- Chapter 1.5: Evaluation of the pressurization conditions on the Aircraft C130 In: C1-30 investigators handbook. Lisboa, Portugal: Instituto Superior Tecnico; 2017.
- [Google Scholar]
- C130J human vibration, Air operations division, Department of Defence, Australian Government Australia: Defence Science and Technology Organization; 2005.
- [Google Scholar]
- Defining the Cockpit noise hazard, aircrew hearing damage risk and the benefits active noise reduction headsets can provide. RTO-EN-HFM-111.
- [Google Scholar]
- Aeromedical evacuation models. Available from: https://www.knightaerosapce.com [Last accessed on 2022 Jul 05]
- [Google Scholar]




