
Translate this page into:
Analysis of medical emergencies in commercial flights and utility of medical resources onboard

*Corresponding author: Avinash Ballekere Krishnegowda, Specialist in Aerospace Medicine, 2 AMTC, Air Force Academy, Hyderabad, Telangana, India. avinas8@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Krishnegowda AB, Dahiya M, Rastogi P, Murthy HM. Analysis of medical emergencies in commercial flights and utility of medical resources onboard. Indian J Aerosp Med 2022;66:27-31.
Abstract
Objectives:
Civil aviation in India is flourishing and has resulted in a substantial increase in air travel. Hence, the increase in the number of in-flight emergencies is not unanticipated. This study attempts to analyze the incidence of medical emergencies that occurred on board in a single major Indian domestic airline and to assess the adequacy of the medical equipment provided in the in-flight emergency kits.
Material and Methods:
A retrospective analysis was carried out of the narrative summaries of all medical events reported by the cabin crew of one major airline in the domestic sector. The data represented an average of 39.9% of total domestic passenger volume from January 2015 to December 2017. An assessment of available medical resources onboard and their utility in managing the medical events was carried out. A comparative study was also attempted on the Directorate General of Civil Aviation (DGCA) recommendations on onboard medical resources and those of other regulatory agencies.
Results:
A total of 221 in-flight emergencies were reported from the sample. Breathlessness (n = 52) was the most common presenting symptom and cardiovascular conditions (n = 68) were the most commonly diagnosed medical illnesses. Four deaths on board were reported. Medical kits recommended by DGCA, India, are comprehensive and carry most of the required medications.
Conclusion:
Civil aviation in India is growing with more citizens using airlines for regular commutes and, hence, the likely incidence of more in-flight emergencies. A standardized system for reporting all in-flight medical emergencies, including their outcomes, should be made available to have a better understanding of the problem statement and guide suitable mitigating actions.
Keywords
In-flight medical emergency
Onboard medical resources
Flight diversion
Civil aviation

INTRODUCTION
Over the years, civil aviation in India has shown an expansive growth with even the elderly and individuals with chronic medical conditions frequently opting to fly. Therefore, the incidence of in-flight emergencies is also expected to rise. In-flight medical incidents during commercial air travel, though common, are not often properly studied and analyzed. Commercial airlines regularly record all medical emergencies occurring in-flight. However, it is not obligatory by law, and the data format is not standardized across all airlines.[1]
Directorate General of Civil Aviation (DGCA)[2] has made the provision of first aid kits mandatory in all Indian registered aircraft. Transport aircraft carrying more than 20 passengers are additionally equipped with physician’s kits containing life-saving drugs and aircraft with 30 passengers or more must carry automatic electric defibrillators. Due to the non-availability of evidence-based epidemiological data, the contents of these kits are predominantly guided by anecdotal evidence and experts’ opinions. This study attempts to analyze the incidence of medical emergencies that occurred on board in a single major Indian domestic airline and to assess the adequacy of the medical equipment provided in the in-flight emergency kits. The kit containers are green in color with a white cross and are always sealed. Periodic examination of the kit contents is conducted once a year or in case of opening of the seal. In addition, there is also a provision for a universal precaution kit (UPK). Contents of this UPK are used to clean up any potentially infectious body contents such as blood, urine, vomit, and feces.
MATERIAL AND METHODS
The narrative summaries of all medical events reported by the cabin crew of one major airline in the Indian domestic sector were reviewed. The data represented an average of 39.9% of total domestic passenger volume from January 2015 to December 2017. The narratives comprised medical problems, flight phase when a medical event occurred, care given, usage of medical and first aid kits, action taken concerning flight status, and availability of onboard assistance.
Each case was analyzed and categorized into the most common symptoms and the system involved. Further, based on the diagnosis made by doctors (both onboard and airport doctors) and treatment given and the outcome, the symptoms were categorized under specific body systems. The phase of flight in which the event occurred was also reviewed, and for ease of analysis, the cases of Turn Backs, Diversion, Priority Landing, and “Offloaded in Transit” were considered in-flight emergencies because only these cases warranted the use of onboard resources.
A review of DGCA recommendations for the contents of the first aid kit, physician’s kit, and UPK was carried out and a comparison was drawn with similar kits recommended by the Aerospace Medical Association (ASMA) of the USA and European Aviation Safety Association. The number of cases where first aid kit, physician’s kit, AED, and oxygen cylinders were used was also recorded. The acquired data were then applied to assess the usefulness of medical equipment available onboard in managing medical events.
RESULTS
Total passengers carried by airline during the 3 years duration of the study (January 2015–December 2017) were 96,780,619 and total hours flown were 911,250 h. The average revenue passenger kilometer (rpk) for 3 years was 36.81 billion.[3] During the study period, a total of 221 in-flight emergencies were reported from this single domestic airline company. The data included medical events of 157 male passengers, 49 female passengers, 10 infants, and five airline crew. The incidence rate was calculated to be 3/ million passengers, 2319.5 flights/emergency, and 6 cases/ billion rpk.
The common presenting symptoms and conditions are represented in [Figures 1 and 2], respectively. Breathlessness (n = 52) was the most common presenting symptom followed by unconsciousness (n = 38), uneasiness (n = 35), seizures (n = 33), and chest pain (n = 24). Among the medical conditions identified and post in-flight care given, cardiovascular conditions (n = 68) were the most common followed by anxiety (n = 30) and epilepsy (n = 29). Death on board reported was four in number. One hundred and twenty-two passengers were already known cases of systemic comorbidities. The most common conditions were coronary arterial diseases (n = 28), epilepsy (n = 24), bronchial asthma (n = 21), hypertension (n = 13), and diabetes (n = 12).

- Common presenting symptoms in-flight.
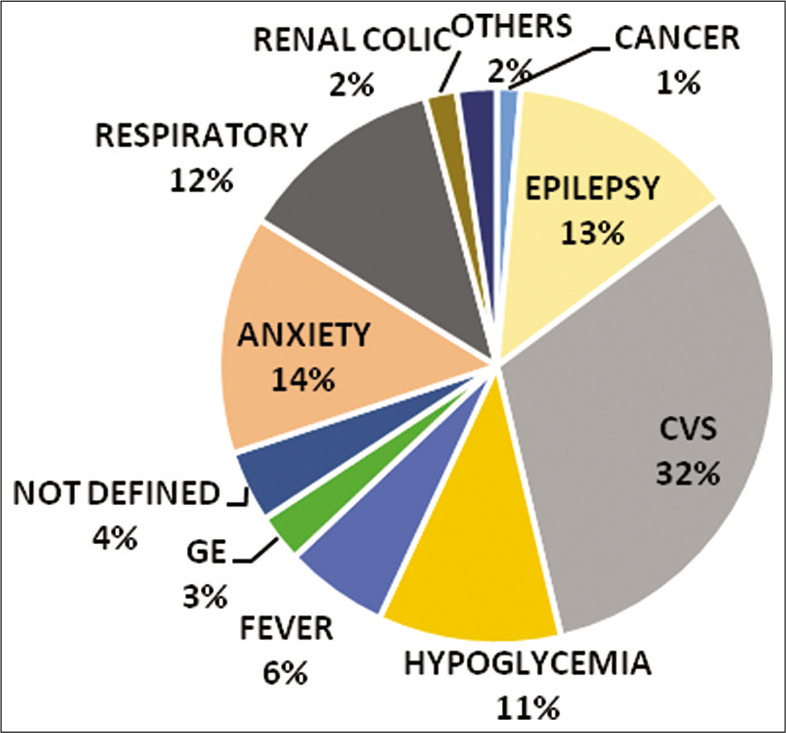
- Common medical conditions in-flight.
The availability of doctors was observed in 141 cases (64%). Nurses and other healthcare professionals were the main responders in two cases each. The crew handled the situation by themselves in 75 cases (34%). O2 cylinder, first aid kit, and medical kit were used in 413,731 cases. AED was used in four cases.
DISCUSSION
The reported incidence of emergencies in the present study was found to be 3/million passengers and 2319.5 flights/emergency. A 3-year retrospective study by Peterson et al. reported one in-flight medical emergency/604 flights.[4] Another study by Dowdal et al. found the incidence of medical emergencies to be 1/11,000 passengers.[5] In terms of cost analysis, the present study found that there was an incidence of six cases of medical emergencies/billion rpk. Sand et al.[6] retrospectively analyzed incidents from two airlines over 5 years and reported an incidence of 14 medical emergencies/billion rpk. Analogous to the same was an analysis by Hung et al.,[7] which included a 5-year retrospective analysis of data of all the telemedicine consultations requested by a single commercial airline wherein the authors demonstrated an incidence of 11.6 cases/billion rpk. Very low incidence rates were observed in the current analysis in comparison to other studies. A plausible explanation would be underreporting coupled with a lack of standardization in data collection and storage.
Unconsciousness and breathlessness have been among the common medical symptoms reported by various researchers. The most common medical emergency (37.4%) in a study by Peterson et al. was syncope or presyncope.[4] The data presented by Sand et al.[6] also indicated that syncope was the most common in-flight event. However, Baltsezak et al.[8] reported gastrointestinal symptoms to be the most common. Similarly, Qureshi et al.[9] demonstrated that respiratory symptoms were most common, and usually, these were due to exacerbation of the pre-existing disease. In our study, the most common in-flight symptoms were breathlessness and exacerbated preexisting diseases were cardiovascular in origin.
The contents of physician’s kits and first aid kits are mandated by DGCA, India.[2] The drugs contained in the physician’s kit are intended to be administered only by a qualified medical practitioner whenever available onboard the flight. In comparison with similar kits recommended by ASMA of the USA[10] and the European Aviation Safety Association,[11] the DGCA recommended first aid kit is more comprehensive and contains all medications required for handling minor medical problems in-flight. EASA additionally recommends usage instructions for drugs along with side effects in a minimum of two languages. EASA does not recommend UPK for medical requirements, however, caters to bio-hazard disposable bags in first aid kit. The physician’s kit recommendations of DGCA and ASMA are similar except for the provision of a separate drug kit by ASMA which contains over-the-counter medications to be used passively, that is, only given to passenger on specific request by the passenger. In comparison to DGCA, EASA recommends the usage of intubation sets and anti-arrhythmic drugs in a physician’s kit. We found these to be useful additives since breathlessness and chest pain was reported as the most common presenting symptoms in the present study. EASA also recommends a delivery kit as a component of a physician’s kit.
In the present study, breathlessness (23%) was reported as the most common presenting symptom and oxygen cylinders available onboard were utilized frequently. The provision of a handheld pulse oximeter would help in arriving at a probable diagnosis and effective management of emergencies in such cases. Irrespective of the actual flying altitude, the cabin pressurization is usually kept at an equivalent range between 6500 and 8000 feet. Due to this, a healthy passenger who is asymptomatic may also show pulse oximeter readings below 94%. This natural change in physiology should be made aware to the healthcare provider before one uses a pulse oximeter in the aircraft cabin. Furthermore, four out of 10 pediatric emergencies had respiratory symptoms. Similar findings have also been brought out by Moore et al.[12] Hence, it is prudent to add disposable pediatric masks for inhalation as a mandatory component.
The present study reported 23 cases of hypoglycemia out of which 12 had pre-existing diabetes. Unconsciousness (17%) was the second most common presenting complaint. Hypoglycemia can cause altered mental status and blood glucose monitors are not part of emergency medical kits. Observing this, Nable et al. recommended the use of blood glucose meter in the aircraft for the passenger in distress.[1,13] This study also reported that almost 1/3rd of medical emergencies were of cardiovascular origin. Hence, addition of statins and clopidogrel along with aspirin as a precautionary measure to manage cardiac event could be considered. The cabin crew members are trained regularly in handling and identifying cardiovascular conditions, but stethoscopes and sphygmomanometers are made available only in medical kits which they cannot open. Besides, the medicines in the medical kit are all injectable only which needs skill for administration. Moreover, both first aid kit and physician’s kit are always sealed and need reporting on opening irrespective of who uses it. Thus, provision of single medical kit with separate compartments for injectables and equipment may be explored. Female passengers who develop menstrual bleed can be assisted by provision of sanitary napkins in the UPKs. First aid kits have an anti-spasmodic, but provision of tranexamic acid or equivalent would also be beneficial in controlling excessive menstrual bleeding onboard.
The aisle space recommendation by EASA between two seat rows in commercial airlines is between 15 and 25 inches.[11] A medical kit/first aid kit commonly used is essentially a briefcase that mirrors out horizontally when opened thus, consuming more space and restricting the ease of usage. The portability of the kit within the aircraft once opened is also cumbersome. A comprehensive kit with a wheeling facility and vertical opening capacity may be investigated.
The cabin crew is one of the most vital resources on board an aircraft as they are mediators between pilot and first care responders. A trained cabin crew can assist in patient care and also help in decision-making for aircraft diversions. According to the DGCA, all crew members must receive initial and periodic training for basic emergency medical events, including AED use, every 24 months.[14] Since all crew members are made familiar with the proper function, usage, and location of the emergency medical equipment, early and optimal care for sick passengers would be ensured.
Many airlines in developed countries are now using “telemedicine” to augment patient care during in-flight emergencies. During our interaction with airline medical doctors, we learned that Indian airline companies also utilize this facility while operating overseas. This provides a link from the aircraft to a ground station where medical advice may be given, often based on information transmitted from the aircraft (e.g., ECG data and pulse oximetry, images of the patient, and two-way communication).[15] An effective telemetry system can aid in rapid and judicious decision-making for diversions.
Attempting to evaluate and possibly treat a sick passenger onboard a commercial aircraft poses many difficulties, namely, there may be little or no information about the patients existing comorbidities, the aircraft cabin offers little space for comfortable clinical examination, aircraft turbulence, and noise from the engine or other fellow passengers. Various researchers recommend that the physician must direct clinical intentions toward stabilizing the patient’s symptoms instead of attempting an absolute diagnosis and duly suggest to the aircrew if diversion is needed. Ethically, a medical professional should volunteer whenever a medical emergency is announced. The major reason for hesitation in volunteering may be legal ramifications. In the USA, the Aviation Medical Assistance Act protects fellow passengers from unlawful legal suits in case they offer medical assistance in-flight. Conversely, in India, a Gazette Notification published in May 2015 protects a good Samaritan who offers help in case of road traffic accidents.[16] Notwithstanding this, whenever possible a doctor should always take valid consent from the patient or his relative before proceeding with medical care. If the care was provided, a written record of events is to be maintained, and the same is to be provided to the airline and to ground medical staff.
The present study had a few limitations. The narratives recorded were not standardized; hence, there was a lack of information on patient particulars, milder emergencies that were handled successfully, medical conditions of the crew who reported sick, and the type of medicines used. Information about the duration of the flight, number of take-offs and landing, and in-flight duration before the emergency were also not retrievable.
CONCLUSION
Civil aviation in India is growing with more citizens using airlines for regular commutes. This increased strength in passengers also brings with them more existing comorbidities which may get exacerbated in-flight. During the study period of 3 years, a total of 221 in-flight emergencies were reported from this single domestic airline company. The common in-flight symptoms reported were breathlessness, unconsciousness, uneasiness, seizures, and chest pain. Cardiovascular conditions were the most common cause of in-flight medical emergencies. A standardized system for reporting all in-flight medical emergencies, including the following outcomes, should be made available, to better guide interventions in the future. The medical resources available onboard were found to be comprehensive and comparable to those recommended by other regulatory agencies.
Acknowledgments
The authors sincerely acknowledge the help and support rendered by Col (Rtd) KN Rao, CMO Indigo Airlines, Gp Capt R Rajesh, DMS (CA), Gp Capt P Pant JDMS (CA), Wg Cdr N Katoch JDMS (CA), and Dr. Kailash, CMO Jet Airways, Delhi sector.
Declaration of patient consent
Patient consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- In-flight medical emergencies. Western J Emerg Med. 2013;14:499-504.
- [CrossRef] [PubMed] [Google Scholar]
- Section 2 Airworthiness series “x” Part III, dated 12th June 1997. Effective: 15th February 2001; Provision of first Aid Kits and Physician's Kit in Aircraft New Delhi: Government of India, Office of the Director General of Civil Aviation; 2001.
- [Google Scholar]
- Handbook on Civil Aviation Statistics 2016-17 New Delhi: Government of India, Office of the Director General of Civil Aviation; 2017.
- [Google Scholar]
- Outcomes of medical emergencies on commercial airline flights. N Engl J Med. 2013;368:2075-83.
- [CrossRef] [PubMed] [Google Scholar]
- Is there a doctor on the aircraft? Top 10 in-flight medical emergencies. BMJ. 2000;321:1336-7.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical and medical emergencies on board European aircraft: A retrospective study of 10,189 cases. Crit Care. 2009;13:R3.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors of flight diversions and deaths for in-flight medical emergencies in commercial aviation. Arch Intern Med. 2010;170:1401-2.
- [CrossRef] [PubMed] [Google Scholar]
- Clinic in the air? A retrospective study of medical emergency calls from a major international airline. J Travel Med. 2008;15:391-4.
- [CrossRef] [PubMed] [Google Scholar]
- Medical Guidelines: Aerospace Medical Association Air Transport Medicine Committee, USA 2016.
- [Google Scholar]
- Pediatric emergencies on a US based commercial airline. Pediatr Emerg Care. 2005;21:725-9.
- [CrossRef] [PubMed] [Google Scholar]
- In-flight medical emergencies during commercial travel. N Engl J Med. 2015;373:939-45.
- [CrossRef] [PubMed] [Google Scholar]
- Section 7 Training and Licencing Series “M” Part I, Dated 15th Mar 2010 Cabin Crew Training New Delhi: Government of India, Office of the Director General of Civil Aviation; 2010.
- [Google Scholar]
- Ministry of Road Transport and Highways Notification Dated 12 May 2015 New Delhi: Government of India;
- [Google Scholar]




