
Translate this page into:
Accident of a civil passenger aircraft at a military airfield: The Casevac experience

*Corresponding author: Dr. R Sarkar, MBBS, MD, Department of High Altitude Physiology and Hyperbaric Medicine, Institute of Aerospace Medicine, Bengaluru- 560 017, Karnataka, India. sarkar.riddhi@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sarkar R, Mohapatra SS. Accident of a civil passenger aircraft at a military airfield: The Casevac experience. Indian J Aerosp Med 2019;63(2): 96-101.
Abstract
Introduction:
There are many civil airports in India wherein the airfield and flying operations are controlled by the military whereas, the Airports Authority of India (AAI) controls the civil terminal. Accident of a civil aircraft on such a base poses unique challenges. This paper discusses the medical contingency plan of a Naval Air Station to deal with civil aircraft crashes based on a civil aircraft incident.
Case Details:
In the early morning of late Dec in 2016, a Mumbai bound civil flight (Boeing 737) took off from an Indian Navy controlled airfield. While initiating the take-off roll from RW, it veered off the runway towards right and came to halt along the perimeter road 230 m north of the runway edge, on hard rocky ground. There were 154 passengers and 7 crew members who were evacuated from the aircraft, through emergency chutes. Few passengers escaped through the over wing hatches. Twenty passengers sustained injuries, mostly involving the lower limbs. This was primarily due to jumping on hard rocky ground and falling and tripping on rocks while moving away from the aircraft. An analysis was done to understand the limitations on the existing medical contingency plan.
Discussion:
The ICAO Airport Services Manual Part 7 on Airport Emergency Planning (Doc 9137-AN/898 Part 7) is the guiding reference for all airports on Airport Disaster and Planning. The Medical Services portion delineates clearly the role of the Medical Aid Providers. In the instant case, the medical department had successfully handled the casualty evacuation and their medical management. SOP and the existing medical contingencies were effectively used. A post-accident analysis in the instant case revealed that 17 out of 25 checklist points were satisfied. The lessons learned from the incident have been discussed in the paper.
Keywords
ICAO
Medical contingency
Boeing 737

INTRODUCTION
Certain airfields in India are defence controlled, wherein crash, salvage, and air traffic control (ATC) are controlled by collocated military airbase and the civil terminal operations are handled by Airports Authority of India (AAI). Apart from ATC and runaway control, these airbases provide crash and salvage and emergency medical cover to civil air operations. The military airbase referred in this article is one of the busiest airports of the Western India due to constant tourist movement involving both domestic and international civil air operations apart from its routine military air operations.
Contingency planning
The primary objective of dealing with aircraft accident is to act with utmost speed and take prompt action to save valuable lives, costly aircraft, and public property. It is, therefore, imperative to set forth detailed procedures for each type of emergency so that each individual organization would act promptly exercising sound judgment and take initiative while dealing with the type of emergency. The air station contingency planning is the process of preparing an airport to cope with an emergency occurring at the airport or in the vicinity or any remote inaccessible place such as forest, mountain, or high seas. In general, a majority of accidents occur during takeoffs and landings, which are either within the airport boundary or a little distance from it. The main object of such a plan is to minimize the effects of an emergency, particularly in respect of saving lives and maintaining aircraft operations.[1-4]
Scope of responsibility
In case of a civil aircraft accident, the medical scope and responsibility are as follows:[5,6]
In case of an aircraft accident inside the airfield, the concerned military air station undertakes the task of providing the immediate first aid and security. Further, the seniormost medical officer becomes overall in charge at the crash site for providing medical aid until the arrival of state medical authorities from Director Health Services.
In case of an aircraft accident taking place outside the airfield limits, the military air base continues to coordinate all post-accident actions. Although the responsibility of providing medical aid remains with state medical authorities (Director Health Services), the air station provides them the assistance to the fullest.
Since the number of passengers involved in civil aircraft is larger and cannot be handled by military air base alone, Director Health Service would provide all medical aid in both the situations as mentioned above para (a) and (b).
Invariably, the seniormost medical officer of the military airbase becomes the overall in charge of the medical arrangements. He continues to liaise with the civil medical authorities (Director Health Services) and organizes for the prompt evacuation of causalities to the respective medical centers. In addition, airport authority and the affected airline operator requisite ambulances/ suitable vehicles and direct them to be available at the discretion of crash site medical officer.
CASE DETAILS
Incident
At about 0504 h of the fateful day, one civil passenger aircraft (Boeing 737), while initiating takeoff roll from runway, veered off the runway toward right and came to halt along the perimeter road 230 m north of the runway edge on hard rocky ground.

Casualty evacuation
There were 154 passengers and 7 crew members who were evacuated from the aircraft, through emergency chutes. A few passengers escaped through the overwing hatches. The injuries sustained by the passengers were mainly due to jumping on hard rocky ground and falling and tripping on rocks while moving away from the aircraft. A total of 20 casualties with no fatalities or head injury were received. Most of them had suffered from lower limb injuries due to jumping from a height and landing on the uneven ground apart from tripping and falling during the emergency evacuation. Two pregnant ladies, one with mild spotting, were also among the passengers. The medical facilities involved in the Casevac operation were as follows:

-
Ambulances
Service ambulance from station: 2 (aa) Crash ambulance (with ATC): 1 (ab) Medical inspection (MI) room ambulance: 1
Ambulance ex-service hospital: 1
Ambulance ex-AAI: 1.
-
Medical officers
At site: 3
Medical officer for back up at MI room: 2
Medical Assistants (paramedics): 10.
-
Emergency medical aid
-
On-site
(aa) All uninjured passengers and crew were made to assemble near the glide slope building about 200 m from crash site
(ab) Triage and prioritization for injured were carried out on the spot
(ac) Minor injuries such as abrasions and scratches were treated at site
(ad) After providing necessary first aid, all Priority II cases were dispatched through the MI room to the nearest hospitals (empanelled private hospital)/ nearest civil government hospitals
(ae) Priority III cases were evacuated to air station Medicare Centre
(af) All passengers and crew were provided water and comforted with request to remain calm as there was no immediate danger to anybody as well as the aircraft. These uninjured passengers were subsequently transferred to terminal building by airport buses.
-
Treatment at air station MI room. There were 20 Priority II and III casualties. All of them were evacuated to air station Medicare Centre and treated as follows:
(aa) Four cases with lacerated wound (PIII). Managed by suturing and antiseptic bandaging
(ab) Ten cases with abrasion (PIII). Managed by antiseptic bandaging
(ac) Two cases with extreme anxiety (PIII). Treated with oral anxiolytics
(ad) Two cases with bony injuries (PII). Two casualties had suffered from bony injuries (one with fracture right patella and the other with fracture left elbow). Both were immobilized with Thomas and Kramer–Wire splints and were administered IV analgesics and later transferred to the civil hospital.
(ae) Two passengers with pregnancy (PII). Two lady passengers in their third trimester of pregnancy were also evacuated.
-

One complained of exhaustion and the other complained of mild spotting, as they slid down the emergency chutes. They were examined clinically along with monitoring of blood pressure and fetal heart rate. They were also referred to the nearest civil hospital.
Timelines
Within 10 min of crash, DMO and the crash ambulance reached the crash site and within 20 min all Priority II cases were attended, completed the triage and initial stabilization on-site and then evacuated to air station Medicare Centre. Within an hours time, the entire process of casualty evacuation to various civil hospitals using service ambulances and ambulances provided by AAI, was completed.
DISCUSSION
Post accident analysis
The ICAO Airport Services Manual Part 7 on Airport Emergency Planning (Doc 9137-AN/898 Part 7) is the guiding reference for all airports on airport disaster and planning.[7] The medical services portion delineates clearly the role of the medical aid providers. To arrange adequate quantity of emergency store and supply to cater various contingencies, a guiding principle is used to prepare the list called List 3-1 [Figures 1 and 2].[7]
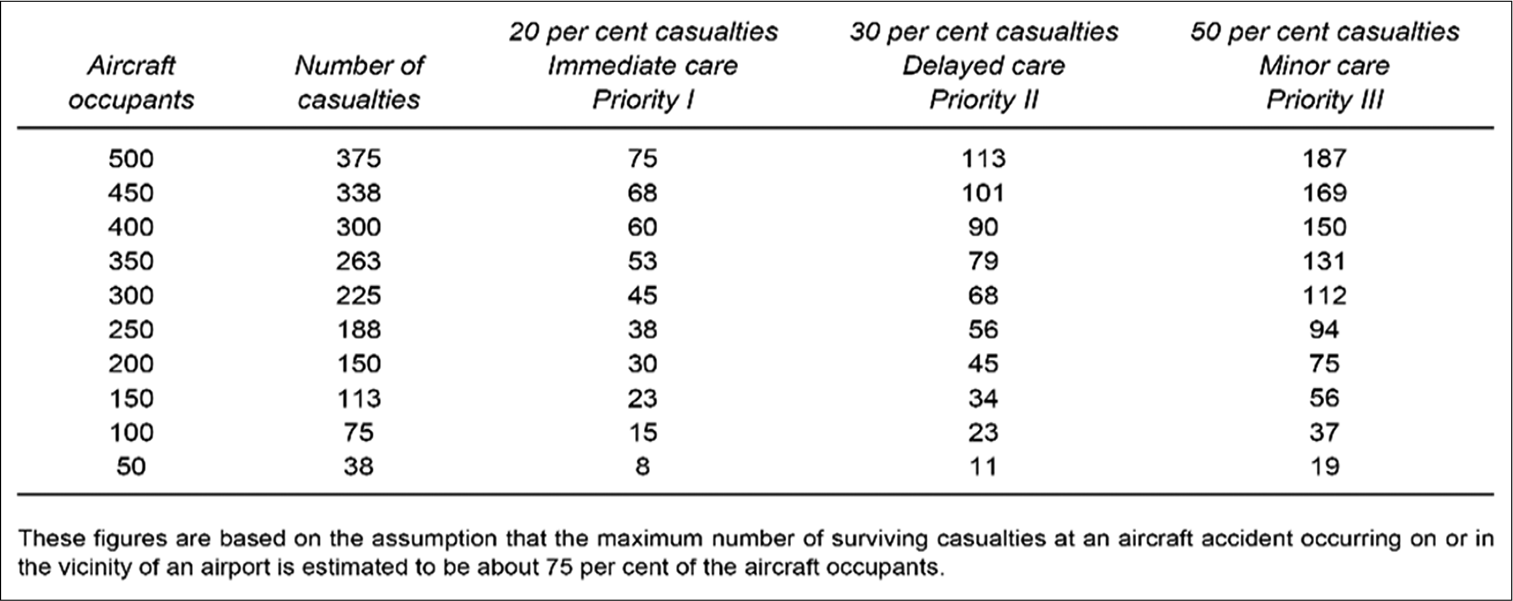
- Estimated maximum number of casualties in an aircraft accident in vicinity of an airport.
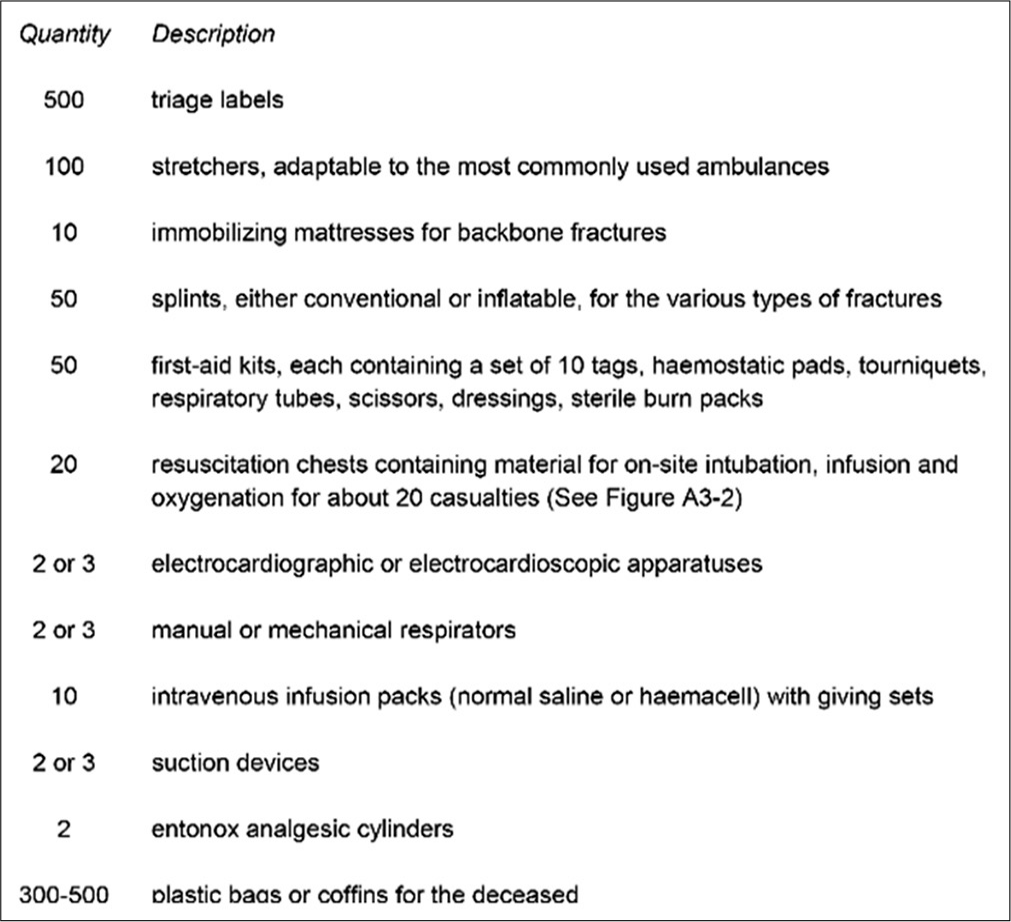
- List of general emergency supplies.
Statistical data collected from aircraft accidents across the globe indicate that about 75% of the aircraft occupants are expected to be surviving casualties with 20% as Red (Priority I) needing immediate care, 30% as Yellow (Priority II) needing delayed care, and 50% could be with minor ailments under the category Green (Priority III).[7]
Observations
The following Table 1 enumerates the extent of utilization of the existing SOP during the above-mentioned aircraft emergency. Of the 25 recommended checklist points, the compliance was satisfied in 17. The points which could not be followed or adhered were listed as the “Lessons Learnt” and the same were recommended for inclusion in the existing SOP.
| Actions | ||
|---|---|---|
| Recommended | Actions taken | Remarks |
| Provide triage | ✓ | Triage done on-site |
| Stabilization of serious injuries | ✓ | Provided on-site as well as at MI room |
| Provide first aid to minor injuries | ✓ | First aid to all was provided at MI Room |
| Transportation of casualties to hospitals | ✓ | Casualties transported to government hospital and nearest civil hospital |
| A medical coordinator for the control of emergency medical operations | ✓ | Seniormost medical officer of the military air station |
| Ambulance services | ✓ | Available |
| Medical transportation officer | ✓ | Chief ward master, MI room |
| Accounting for casualties | X | Few Priority III casualties who left in the first ambulance could not be accounted for |
| Coordination with emergency medical assistance system in the region | ✓ | Catered in civil aircraft contingency plan of the military air station |
| Emergency medical communication system | X | There is no separate emergency medical communication system. There are adequate number of Motorola sets which are common channels for the air station |
| Training | ||
| Training of personnel in emergency medical procedures | ✓ | All the personnel assigned to rescue duties trained in first aid and CPR |
| Periodic exercises and drills | ✓ | Conducted every 6 months |
| Equipment | ||
| Equipment | Ideal quantity | Quantity held |
| Triage labels | 500 | 100 |
| Stretchers | 100 | 15; provision of additional stretchers from empanelled/dependent hospitals |
| Immobilizing mattresses | 10 | Nil |
| Splints | 50 | ✓ |
| First aid kits | 50 | 10 bricks. The first aid material in these bricks is enough to cater for first aid for 50–100 people |
| Resuscitation chests | 20 (should contain material for on-site intubation, infusion, and oxygenation for about 20 casualties) | 5; provision of additional stretchers from empanelled/dependent hospitals. ER cardiac care (one defibrillator and two AEDs) available in enough number |
| Electrocardiographic equipment | 2 or 3 | ✓ |
| Manual or mechanical respirators | 2 or 3 | ✓ |
| Intravenous infusion packs | 10 | ✓ |
| Suction devices | 2 or 3 | ✓ |
| Entonox analgesic cylinders | 2 | Nil: No provision of storage in a non-hospital set up |
| Plastic bags or coffins | 300–500 | 10 |
| Inflatable tents | Nil | One service issue tent is available with the GSARP team; however being a time-consuming procedure, it was not rigged |
CPR: Cardiopulmonary resuscitation, AED: Automated external defibrillator, GSARP: Ground Search and Rescue Party
Lessons learnt
Any aircraft accident leaves a trove of information and knowledge that can be utilized for future prevention and better handling of such events. From the above, it is quite evident that handling of the incident was more than adequate and to an extent, commendable; however, there were valuable lessons learnt which have been incorporated into the existing setup.
Better communication among medical aid agencies
There could have been better communication among the aid agencies. Although concerned agencies of the military base were immediately sounded toward receipt of casualty, it took sometime before AAI could activate its channels of medical aid. Towards this, establishing a separate hotline with the ATC tower and the Airport Manager was considered necessary.
Difficulty in onsite triage and first aid due to darkness
The time of the accident was 0504 h, it was still dark and the aircraft crashed and lodged itself in a dark and desolate part of the establishment which did not have any electrical lighting. The initial first aid was provided in street light. Only one emergency light-emitting diode was available which was inadequate. The Accident Response Kit should have adequate numbers of LED lights to operate at night conditions.
Training of civil agencies (government and private empanelled hospital) in mass casualty handling
There is a civil aircraft crash exercise held by the military air station in coordination with civil agencies on a bi-annual basis.[6] However, this being an actual civil aircraft incident at this airport since 2005,[5] the response of the civil authorities toward the alacrity of the situation, left lot to be desired. The local government hospital will be overwhelmed in case of a large number of Priority I casualties and the nearest government tertiary care center was 25 km from the air base. Increasing the mock up drill and Post Accident Plan exercises with all stakeholders would help in better preparedness to deal with such an eventuality.
Inadequate number of stretcher-bearers and stretchers
Although there were no Priority I and very few Priority II cases, it was felt that the number of stretcher-bearers was inadequate. The number of stretchers held by the unit was also less. Toward this, the nearest service hospital and other armed forces units can be requested to share their resources to fulfill the requirement. The existing facilities and the resources available at AAI also need revision for better handling of such emergencies.
Triage site and casualty holding area
Although the accident did not have any fatalities and the perimeter road and the glide slope building (200 m from crash site) provided adequate space for triage, any fatalities would have proved disastrous from the point of view of evidence collection and casualty evacuation. The building designated for casualty holding in the contingency plan has been converted into a VVIP terminal and cannot be used for the storage of dead bodies and/or crisis management center. A case for expansion of the present medical infrastructure at the military air base has been taken up with concerned authorities.
Enhancement of medical facilities in terminal building
The airport authority is dependent on the co-located military air station for emergency medical care and on local government and private hospitals for empanelment. However, the regulation states that each terminal should have a fully equipped medical clinic and/or a first aid room. The facilities provided by the clinic in terms of trained workforce and equipment should be aligned to ICAO recommendations.
CONCLUSION
A military airfield always remains ready for any aircraft eventuality be it civil or military. The above mentioned accident of a civil passenger aircraft (Boeing 737) provided a unique perspective to all stakeholders toward the approach of civil aircraft crash. It is a providence that there were no fatalities or any Priority I injuries to any passenger or crew. This also provided concerned medical personnel an opportunity to experience an actual crash (ground accident) with enough scope for introspection and audit of their own capabilities and shortcomings. All involved agencies acted with intense urgency and professionalism to handle a potentially catastrophic situation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Airport preparedness for mass disaster: A proposed schematic plan. Aviat Space Environ Med. 1986;57:77-81.
- [Google Scholar]
- Mobilization of trauma teams for aircraft disasters. Aviat Space Environ Med. 1980;51:1262-6.
- [Google Scholar]
- Medical coordination in airport disasters. Aviat Space Environ Med. 1980;51:1256-8.
- [Google Scholar]
- Civil aircraft disaster management on naval air station: Challenges and concerns. Indian J Aerosp Med. 2008;52:65-70.
- [Google Scholar]
- Civil Aircraft Crash Contingency Plan for Naval Air Station
- The ICAO Airport Services Manual Part 7 on Airport Emergency Planning, Doc 9137-AN/898 Part 7 Montreal: International Civil Aviation Organization; 1991.
- [Google Scholar]




