Translate this page into:
A preliminary study on empathy and personality in military medical officers
Abstract
Empathy forms the integral part of rapport in the doctor-patient relationship. It refers to understanding the other person's inner experiences and communicating the same. This has been found to be an important facet in patient care. Physician empathy has proven to be effective in enhancing patient satisfaction, improving their compliance and also increasing the physician's efficiency to diagnose and treat patients. It is all the more crucial for military medical officers to be empathic with their patients and understand the stress inherent in military life due to such factors as occupational requirements, stringent work schedules and discipline. Operational missions by the forces during war or peacetime necessitate exemplary physical health coupled with impeccable precision in mental processes. Empathic approach aids in the accurate assessment of overall fitness there by increasing the operational efficiency. A preliminary study was conducted to measure the level of empathy in a sample of medical officers and the association between empathy, personality attributes and demographic variables. 119 medical officers were administered self-report questionnaires, such as the 16 PF test, Jefferson's Scale of Physician Empathy, Marlowe Crowne Social Desirability Scale and a demographic inventory. Scores were statistically analyzed using the Student t-test, ANOVA and Pearson's product moment correlation. Results indicated an average level of empathy in this sample. Empathy was significantly correlated with some personality characteristics such as abstract intelligence, sensitivity and self concept control. A significant negative correlation with education was observed. Significant gender differences were observed in empathy, and the personality variables of enthusiasm and tension. Results have implications on the selection and training procedures of military medical officers to further enhance the quality of medical services.
Keywords
Empathy
Personality
medical officers

Enduring human relationships have their basis in mutual trust, care, concern and understanding. Healthy interactions, laced with good communication and empathic behavior are essential for strengthening interpersonal relationships. “The secret of the care of the patient is in caring for the patient” where the term caring takes larger than life magnitude. “Treatment of disease may be entirely impersonal but the care of patient must be completely personal” [1], which highlights the value of personal bonding in doctor-patient relationship, for better clinical outcomes.
A predominant component of satisfying doctor-patient relationship is empathy [2]. The origin of the word empathy is from a Greek word empathies meaning affection or passion with a quality of suffering. “Em” means “into”, “pathos” from the Latin means “feeling” or “perception” [3] In the layman's understanding, empathy is the ability to place oneself in another's shoes [4]. In the health care scenario, it is defined as 'a cognitive attribute that involves an understanding to the inner experiences and perspectives of the patient combined with the capability to communicate the same to the patient' [5]. Empathy, however, as a unique concept, manifests itself in 3 stages; cognitive, affective and behavioral. An empathic physician has the cognitive capacity to understand the patient's needs and the affective sensitivity to feel the same, as well as the behavioral ability to convey and communicate the same to him [6].
Empathic concern by the physician has been proved to improve patient's compliance [7,8,9,10] and satisfaction [9, 10, 11]. An empathic physician who is emotionally sensitive to the patient's problems develops the capacity to diagnose more accurately, speeding up the healing process for better therapeutic results [4,9,12]. Empathy plays a vital role in promoting professional excellence[5]. A study pertaining to the personal characteristics that distinguish compassionate empathic physicians from other physicians emphasizes empathic measures as one of the most important prerequisite personality quality for a good physician [13].
In the military services personnel are constantly exposed to multifarious stressors which are more severe and intense as compared to the stressors encountered in civil. This apart, due to imposed discipline and lack of opportunities for verbal expressions, the personnel are emotionally more inhibited and need proper care, concern and understanding of their problems. Therefore the role of empathy is much more important. In the military context, leaders need to be empathic in dealing with their subordinates [14].
Empathy, as an integral part of the patient care, goes a long way in ascertaining the efficacy of military medical officers in understanding the problems encountered by the military personnel. This becomes more meaningful, when they deal with them either during peacetime or combat operations. In this context, an empathic military medical officer, plays a consequential role, by evaluating the enormity of the stresses, reducing the difficulties faced by the concerned, by providing maximum empathy based psychological support and for improved operational efficiency. In a military set up it is speculated that, the hierarchy, rank structure and stringent rules detracts medical officers' from free and close association with the lower ranks. This may restrict communication and restrain empathy. In bureaucratic organizations such as the military, medical professionals are pressurized to adjust their traditional hierarchy of values to conform to that of the organization rather than for a particular patient [15]. This is likely to bring about changes in the doctor's attitude towards the patient, which may even influence his/her empathic level. Military clinicians find soldier-centered approaches problematic, where the problems faced by the soldiers are to be carefully studied by the clinicians and an empathic, compassionate approach has to be employed to solve their problems. This is perceived as a threat to his/her own officer status [16].
In the Air Force, the health of the crew members during the hazardous conditions of the operational environment become the responsibility of a medical officer, in that, he should evaluate the hazard and advise/help accordingly. The importance of the physician-patient relationship is often poorly understood. Rapport with fliers is essential in being able to elicit pertinent medical history [17]. Empathy enhances the trust in the physician [10] and encourages the patient to talk. Lack of empathy may result in lack of disclosure. In the air force, since the flight surgeons are also the medical approval authority for continued flying, pilots may fail to report medical problems for fear of being grounded. Hence a relationship containing the attributes of trust, honesty, openness, shared responsibility, equal concern for flight safety and professional goals becomes mandatory [17,18]. There are value conflicts that arise in medical officers, particularly psychiatrists' as aero medical evaluators, and these can be minimized by recognition, open discussions and thoughtful restructuring of physician- patient relationship [19].
The lower cadres are most often hesitant to approach the physician, for fear of jeopardizing his/ her future as occupational status will ultimately be decided by medical officers. The other repercussions are loss of social status, and financial implications. An un-empathic medical officer with incomplete information about the patient/aircrew may misperceive and misjudge the condition of the patient. In the western countries, the services of psychologists are utilized by the military commanders at all levels including in the field [20]. In India however, military medical officers are expected to provide overall psychological support, in the absence of psychologists.
Measurement of empathy
Individuals differ in their capacity to empathize. This aspect makes it imperative for the development of an efficient tool to measure the empathic ability. Some instruments do exist to measure empathy in general population like the Interpersonal Reactivity Index [21], the Hogan's Empathy scale [22] and the Emotional empathy scale [23]. Earlier, there was no research tool available to measure empathy in doctors and medical students as there was a dearth of empirical research in this field [24]. To address this issue, Hojat et al in the year 2001, developed a scale with reasonable psychometric support [25], to measure level of empathy in physicians and named it the Jefferson's Scale of Physician Empathy (JSPE).
Empathy and Personality
Empathy is often correlated with certain personality attributes. Specific type of personality style is said to be related to clinical success. In a study of medical students using two self-report questionnaires, it was revealed that certain personality, style may be less successful in promoting healthy interpersonal relationships essential for good medical care. Personality profiles with low level of anxiety and phobic concerns and high self esteem may be ultimately related to clinical success [26].
One study [22] showed a negative correlation between certain scales of Minnesota Multiphasic Personality Inventory (MMPI) i.e. depression, social introversion and anxiety on the Hogan's Empathy Scale. There was also a high positive correlation between this scale and subscales of California Personality Inventory and Maudsley Personality Inventory and MMPI subscales measuring social and personal adequacy and extroversion. Studies with Truax Empathy Scale supported these results [27,28]. Empathy was found to be positively correlated with sensitivity and well being and also negatively correlated with depression and anxiety [29, 30]. In a study by Streit [31], medical students were administered Hogan's Empathy Scale and 16 Personality Factor test (16 PF), in an attempt to describe their personality characteristics and changes during medical training. Depressive symptoms were found to be negatively correlated with empathy. Certain factors on 16 PF like being venturesome, tender minded and impulsively lively had a positive relation with empathy. Another study [23] using an emotional empathy scale found that helping behavior was significantly positively correlated with empathic understanding.
Empathy and Demographic Characteristics
Studies have been conducted to show the strong link that exists, between demographic variables such as age, gender, and clinical experience and the degree of empathy. Gender differences in empathy were found in many studies. Females were found to be more empathic than men [2, 5, 24, 31,32]. Eisenbergand Lennon [33] view that the large sex differences favouring women is more evident when the measure of empathy was on self-report scales. They found gender differences were non-existent when the measure of empathy was either physiological or unobtrusive observations of non-verbal reactions to another's emotional state. Clinical experience has also been related to degree of empathy. Studies have reported a decline in empathy in medical students, and faculty over a period of time, which could be attributed to cynicism, cumulative life experiences and part of an adaptive response [32,34, 35].
Although, there are studies available assessing empathy in civil doctors and health professionals, no such attempts have been made to assess empathy in military medical officers both in India and abroad. It is strongly felt that, considering the enormity of the occupational stressors influencing and the work environment, a military medical officer needs to be much more empathic than civil doctors who generally deal with patients who are in less stressful environmental conditions. The aims of this research were to study (a) the degree of empathy in a sample of military medical officers (b) the association between empathy and personality attributes and (c) the association between empathy and demographic variables such as age, gender, and duration of clinical experience.
Material and Methods
Subjects: The participants of this study were 119 medical officers, consisting of : officers who were detailed for primary course in Aviation Medicine at IAM (n =78) from different units; those who opted for the advance course in Aviation Medicine at IAM (n =29); and a group of 11 medical officers who were resident MD course in different medical specialities from Command Hospital, (AF), Bangalore. The subjects consisted of both male and female, married and single, short service commissioned (SSC) and permanent commissioned (PC) officers. They were from all the three wings of armed forces (Army, Navy, and Air Force). A few foreign students from various countries (Nigeria, Sri Lanka etc.), who attended the primary course, were also part of the study. Demographic characteristics are shown in Table 1A and IB.
| Demographic Variable | Group | Number | Percentage |
|---|---|---|---|
| Sex | Male | 92 | 77.3 |
| Female | 27 | 22.7 | |
| Marital Status | Married | 83 | 69.7 |
| Single | 36 | 30.3 | |
| Course | Primary | 78 | 65.6 |
| Advanced | 41 | 34.4 | |
| Type of Commission | Short Service | 44 | 37.0 |
| Permanent | 75 | 63.0 | |
| Service | Army | 45 | 37.8 |
| Navy | C4 | 3.4 | |
| Air Force | 70 | 58.8 |
| Demographic characteristics (yrs) | Group Mean (S.D) |
|---|---|
| Age | 30.28(4.0) |
| Education | 18.85(2.26) |
| Service | 4.81 (2.72) |
| Clinical Experience | 6.35(3.64) |
Psychological Questionnaires
Demographic inventory consisting of personal details pertaining to the officer.
16PF Test (36): Form D of Cattell's 16PF test, with 105 statements was used. The time duration scheduled was (as prescribed by the author) half-an- hour, which was strictly adhered to, with some exceptions, for those who had language difficulty. A little extra time was allowed in those cases.
JSPE (25): The scale has two versions: the student version(S) and the Health Professional version (HP). The latter version was used for this study, as it was felt more appropriate. The scale consisted of 20 statements (10 positive & 10 negative) which were to be assigned ranking, on a 7 point Likert scale depending on the agreement or disagreement: the higher the ranking, more the agreement. There was no time limit prescribed.
Marlowe-Crowne Social Desirability Scale (SDS) (37): This Scale consists of 33 statements which were to be assigned true or false status, as applicable to the individual. No time limit was prescribed.
Procedure
The subjects were first explained about the purpose of the study. It was also made clear that, the results of the tests will neither have bearing on the results of their course, nor on their medical category. Rapport was established with the subjects before the administration of the tests.
The questionnaires were administered in the above mentioned order. The approximate time taken for completing the questionnaires was around 1 hour and fifteen minutes. Separate set of detailed instructions were given before administering each. The importance of answering frankly, without being guarded, was explained. Precautions were taken against imposing the questionnaires on any one by making some of the personal information voluntary. The subjects were well motivated to answer the self-report questionnaires.
Scoring and Statistical analysis
16PF: The responses were computer scored and profiles were obtained.
JSPE: The positive statements were scored from 1 - 7 (strongly disagree - agree) and the negative ones were reverse scored from 7 - 1 (strongly disagree - agree). The scores were added. Maximum score that could be obtained was 140, the higher the score the higher the empathy.
SDS: The answers were scored according to the prescribed key available. Maximum score was 33. Each correct response was given 1 mark. Scores were added; higher scores indicated higher social desirability. Scores from 17 and below were only taken into account for reliability. This test was, basically used, to double check the reliability of responses - the MD (Motivation Distortion) score of 16PF, being the other check.
The resultant scores were subjected to statistical analysis. Student't' test was used to find out the difference between the two groups on demographic variables. ANOVA was used to find the difference between the three forces on empathy scores. Pearson's Product Moment Correlations were calculated to find out the association between personality attributes and empathy and also social desirability scores. Only statistically significant scores were highlighted.
Results
Normative data
The group as a whole was at average level of empathy with a mean of 111.11 and SD of 12.61 (79 Percentile). Normative data for personality, empathy and social desirability variables in the group is shown in Table 2.
| Variable/ Factor | Mean (SD) |
|---|---|
| MD Warmth (A) Intelligence (B) Emotional Stability(C) Dominance (E) Enthusiasm (F) Conscientiousness (G) Boldness (H) Sensitivity (I) Trust (L) Practicality (M) Forthrightness (N) Self Assurance (0) Conservatism (Q1) Self Sufficiency (Q2) Self concept control (Q3) Tension and frustration(Q4) Anxiety Extraversion Alert poiseIndependence Self disclosure Empathy |
5.80(2.38) 4.86(1.90) 5.64(1.66) 5.45(1.78) 6.45(2.00) 5.12 (2.07) 5.59(1.62) 5.06(1.87) 5.26(2.15) 6.66(1.91) 6.04(2.24) 5.98(1.60) 5.63(1.89) 4.79(1.93) 5.64(1.92) 5.79(1.77) 6.60(2.01) 6.21(1.78) 5.31(1.77) 6.06(1.80) 5.98(1.80) 19.34(5.00) 111.11 (12.60) |
Correlation between empathy and personality
Empathy was significantly correlated with personality characteristics such as abstract intelligence, sensitivity and self concept control as shown in Table 3. Graphical representations of each of the correlations are shown in Fig 1-3.
| Personality Factors | Correlation |
|---|---|
| Abstract Intelligence (B) | 0.20 |
| Sensitivity (I) | 0.18 |
| Self concept control (Q3) | 0.28 |

- Correlation between Empathy and intelligence (Factor B)
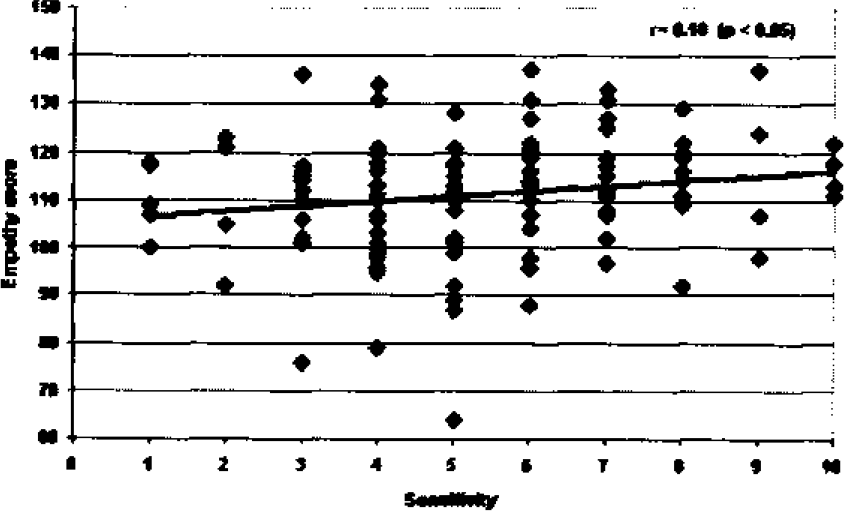
- Correlation between Empathy and Sensitivity (Factor I)
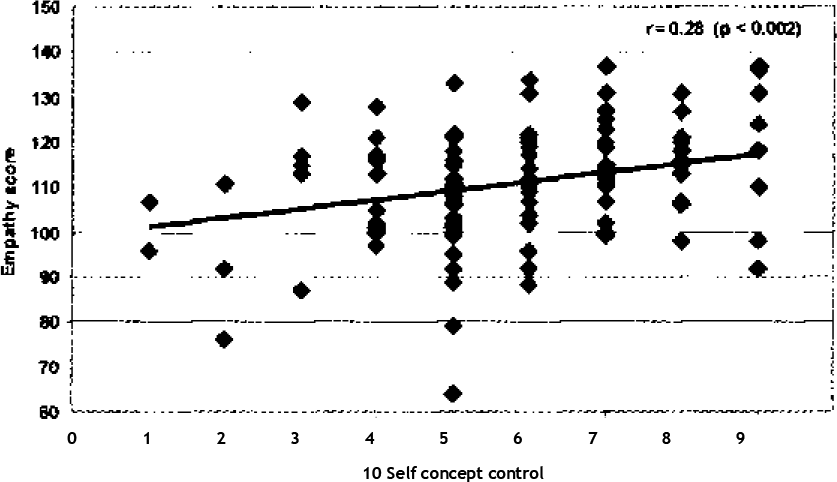
- Correlation between Empathy and Self Concept Control (Factor Q3)
Demographic variables
On the demographic variables, statistically significant gender differences were found in scores on personality factors like enthusiasm, tension and also empathy scores as shown in Table 4.
| Factor | Mean(SD) | 't'value | |
|---|---|---|---|
| Male | Female | ||
| Enthusiasm (F) Tensionistration(Q4)and fru Empathy | 5.53(2.03) | 4.41(2.06) | 2.06* |
| 6.86(1.79) | 5.74(2.49) | 2.17* | |
| 109.6(112.72) | 116.22(10.94) | -2.45*** | |
Differences on other variables were statistically not significant. ANOVA did not reveal statistically significant differences between Army, Navy and Air force officers on empathy scores.
Correlation between empathy and demographic variables
A significantly high negative correlation was observed between education and empathy (r = -0.26; p< 0.004) as shown in the graphical representation (Fig 4). Mean differences and correlations with other demographic variables were not statistically significant.
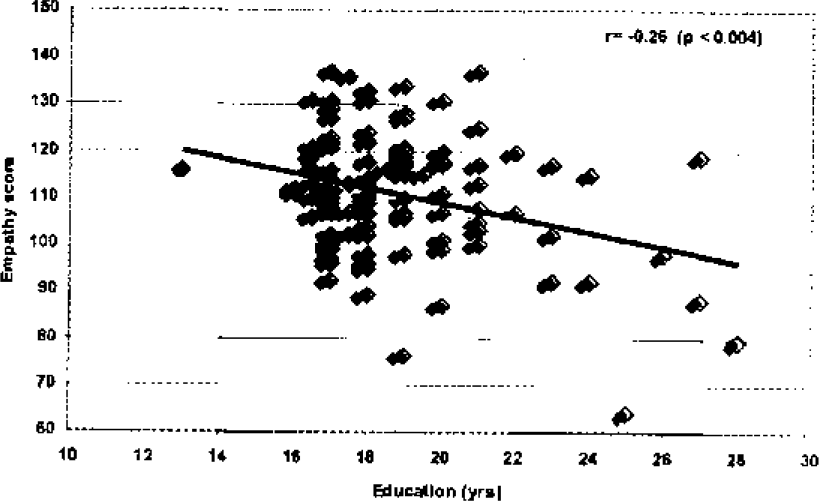
- Correlation between Empathy and Education
Correlation between social desirability and personality variables
Correlations between personality and social desirability (16PF and SDS) indicated a statistically significant negative correlation between trust, self assurance, tension, second order factor anxiety and social desirabi lity. Positive correlations were observed between SDS and MD, self concept control, and emotional stability as shown in Table 5.
| Variable | rvalue |
|---|---|
| MD | 0.48 AAA |
| Empathy | 0.17 # |
| Emotional stability(C) | 0.29 AA |
| Trust (L) | -0.36 AAA |
| Selfassurance(O) | -0.25 A |
| Self concept control (Q3) | 0.32 AAA |
| Tension (Q4) | -0.22 ** |
| Anxiety | -0.40 AAA |
p< 0.0001 AAp<0.002 Ap< 0.007 **p<0.02 #p<0.06
Discussion
The level of empathy, as revealed by the group as a whole, was average. Empathy scores in this group appear to be influenced by social desirability since 67% of the sample, had scores above the cut off score (17/33) and 44 % had an MD sten score of 7 or higher, indicating a tendency of wanting to create a favourable impression on others.
Similar studies on medical students, practitioners and nurses, using the same empathy scale, show comparatively higher empathy levels. JSPE administered on a sample of physicians (n=704) in people oriented specialities (Psychiatry, Gynaecology and Obstetrics) showed a higher average mean of 121.0, where as the technology oriented specialities (Radiology, Pathology etc.) showed a mean of 117.2 [5]. Another study [2], on medical students, correlating empathy and clinical competence showed a mean of 119.0 in men and 122.0 in women. A study, [34] on decline in empathy in medical officers, when administered JSPE to 125 medical students at the beginning and end of 3 years of medical school, showed a mean of 123.1 and 120.6, respectively. Two studies [24, 25] by Hojat et al, showed a mean empathy score of 118.0 and 120.0 respectively, for medical students. A study, where nurses and physicians were compared for empathy scores, showed a mean of 117.2, for the former and 115.7, for the latter [38].
All these studies show that medical students/ physicians/nurses are generally higher on empathy. The variations or the lower level in the mean empathy score in our study, could be attributed to the basic difference in the nature of the sample, in that, they are military medical officers, who, by 1virtue of their rank, position, hierarchy, inadvertently may bring some restraint in their communication, feelings, sensitivity and understanding of the patient. A discussion on how military clinicians should deal with soldiers in army, speaks about the clinicians' perception of soldier centred approaches as problematic since it denies the military reality that the clinician is an officer [16]. This attitude is likely to affect his/her level of empathy.
Several studies have shown that, there is a relationship between empathy and personality characteristics. This study shows a significantly high positive correlation between empathy and personality characteristics such as, abstract thinking, sensitivity and self-concept control. In line with this finding of a positive correlation between abstract intelligence and empathy, Mayer and Geher [39] found that people who are able to identify others emotions are more empathic and intellectually smarter and they concluded that some forms of emotional problem solving requires general intelligence. Two studies [30, 31 ] reported positive correlation between tender mindedness (sensitivity) and empathy, which is also similar to our findings. Empathy fosters self esteem [40] which is an attribute of self concept control. Studies have shown that people with low self control were low on empathy [41].
In one study, Hogan's empathy scale was administered along with another scale measuring depression (both self report questionnaires) to medical students. There was a negative relationship between empathy scores and anxious, obsessive, and depressive clusters [31 ]. The present study did not show a negative correlation between anxiety and empathy. This could be attributed to the nature of the self report questionnaires used. The empathy questionnaire used in this study is used to specifically measure physician empathy whereas Hogan's
Empathy scale may not have been completely relevant to medical fraternity. The other questionnaire used was a clinical scale; whereas our study used 16PF test which measures anxiety as a basic personality trait.
The findings of another study [27] also found similar results. In this, MMPI and Edward's Personal Preference Schedule (EPPS) scores were correlated with empathy scores obtained on Truax Accurate Empathy Scale. Depression, Psychasthenia, Hysteria, and Psychopathic Deviance correlated negatively with empathy. Nurturance and Interception on EPPS correlated positively with empathy. Our study does not corroborate these results, possibly due to the nature of the normal sample, the above study dealt with a neurotic population. One exclusive study on medical students who were administered Hogan's empathy scale and 16 PF test, found traits like being venturesome and impulsively lively, positively correlated with empathy [31]. These results differ from ours, possibly because people in defence services are not generally venturesome, socially bold and spontaneous. They tend to be more emotionally inhibited and cautious, because of the discipline and hierarchy inherent in the military system.
There is a negative correlation between empathy and age. Children are by nature relatively empathic and they slowly lose their feelings of empathy. Research on adolescents and adults seems to support this hypothesis. In our study there is no correlation between age and empathy possibly because our sample consists of adults within a restricted age range.
Our study shows a negative correlation between education and empathy, which implies that education, does not make a person more sensitive to other peoples' feelings. In reality, more educated persons may also tend to be more analytical, rationalizing and intellectualizing, making themselves less sensitive to others' feelings. The higher one goes in the formal education system the more is the emphasis placed on intellectual and cognitive abilities [42].
One study on medical men with Hogan's empathy scale found slight negative changes in empathy with clinical experience which was attributed to cynicism. Empathy was, however, argued to be a stable trait [35]. In this sample, there was no association between empathy and clinical experience, probably the military training and environment restrains empathy, making clinical experience a less important factor.
Empathy and personality factors of enthusiasm and frustration in this study revealed statistically significant gender differences. Females were more empathic than males. This finding corroborates those of several previous studies [2, 5, 24, 31, 32]. Our results show that men are more frustrated than females possibly because cultural gender roles and also the military services allow women to vent out their emotions more than men, leading to higher levels of frustration in them. Men were also more enthusiastic than women, which is a culturally more accepted trait of the male gender role.
Correlation between social desirability, empathy and personality variables yielded certain positive and negative results. The MD score of the 16PF test which indicates the extent of faking -good responses and the social desirability score, referring to the extent of socially approved responses, is highly correlated. This indicates that increased faking good responses results in increased socially acceptable responses and substantiates our previous research on military aircrew [43, 44]. There is a high positive correlation between self concept control and social desirability scores. Cattle [36] defines the self concept control dimension as concern about one's own reputation which is likely to induce socially desirable responses.
Social desirability is positively correlated with emotional stability. Also, this study found that the – higher the socially desirable responses the lower is: he tension, anxiety, apprehension and, suspiciousness. Once again these findings substantiate our previous research on military aircrew [43, 44], Anxious and apprehensive persons are usually more conscious of themselves and less concerned about what others may think, and thus give fewer socially desirable responses.
Conclusions
This study investigated empathy and its association with personality characteristics and demographic variables, in 119 medical officers. A demographic inventory, 16PF test, JSPE and Marlowe Crowne's SDS were administered.
Results were statistically analyzed, and showed an average level of empathy in military medical officers. Personality characteristics like abstract “king, sensitivity, and high self concept control *• r-e positively correlated with empathy. Empathy did not show any significant correlations with demographic variables, except a negative correlation with education. Gender differences indicated that women were more empathic and men were more enthusiastic and frustrated.
This preliminary study has a number of limitations. A detailed analysis of the components of empathy would yield more information. A larger sample size, including different specialties of medicine and different age groups, may yield more specific results. Stability of empathy scores over time could be another interesting aspect of study
This was not looked at here
Recommendation
The results of this study indicate a lower empathy level than similar population samples in previous research; an average level of empathy was observed in this sample of military medical officers. Therefore higher levels of empathy would improve doctor patient communication resulting in an even better quality of medical services. It is recommended that personality attributes such as empathy and emotional sensitivity for healthy communication should be essential requirements for selection of medical officers into the armed forces [31, 26]. Secondly, for officers who are already in the military services, training, which is said to improve empathy and healthy communication, needs to be considered [6, 7, 45]. Sincere efforts should be made to prevent decline in the level of empathy over the years, due to cynical attitudes or any other causes, by conducting indoctrination courses periodically. This will bring about awareness of the importance of being consistently empathic in doctor patient relationships and will also contribute towards self growth.
References
- Empathy in medical students as related to academic performance, clinical competence and gender. J Med Edu. 2002;36:1-6.
- [Google Scholar]
- The empathy cycle: refinement of a nuclear concept. Journal of Counseling Psychology. 1981;28(2):91-100.
- [Google Scholar]
- The importance of empathy as an interviewing skill in medicine-A commentary. JAMA. 1991;266(13):1831-2.
- [Google Scholar]
- The Jefferson Scale of Physician Empathy: further psychometric data and differences by gender and specialty at item level. Acad Med. 2002;77(10):558-60.
- [Google Scholar]
- Empathy training to improve physician-patient communication skills. Acad Med. 1995;70(5):435-36.
- [Google Scholar]
- Empathy in the doctor-patient relationship, skill training for medical students. J Med Educ. 1977;52:752-7.
- [Google Scholar]
- Communicating information to patients-patient satisfaction and adherence as associated with resident skill. J Fam Med. 1988;26:643-7.
- [Google Scholar]
- Doctor-patient communication: the Toronto consensus statement. BMJ1991;. ;303:1385-7.
- [Google Scholar]
- The effect of physician behavior on the collection of data. Ann Intern Med. 1984;101:692-6.
- [Google Scholar]
- Compassionate-empathic physicians: personality traits and social-organizational factors that enhance or inhibit this behavior pattern. Soc Sci Med. 1996;43(8):1253-61.
- [Google Scholar]
- The captive professional: bureaucratic limitations in the practice military psychiatry. J Health SocBehav. 1969;10(4):255-65.
- [Google Scholar]
- Accessed March 7 2008www.pdhealth.mil/clinicians/downloads/tips.pdf
- A survey of the flight surgeons' rapport with the pilot. Aviat Space Environ Med. 1995;66:15-9.
- [Google Scholar]
- Jones DR. The individual's vs the organizations dotcom value conflict in psychiatric aero medical evaluation. Aviat Space Environ Med. 1981;ll(52):04-06.
- [Google Scholar]
- Operational Psychology: An emerging sub discipline. Mil Psychol. 2006;18(4):269-282.
- [Google Scholar]
- Measuring individual differences in empathy: Evidence for a multidimensional approach. J of Pers and Soc Psychol. 1983;44:113-126.
- [Google Scholar]
- Development of an empathy scale. J Consulting and Clinical Psychology. 1969;33(3):307-16.
- [Google Scholar]
- Physician empathy: Definition, Components, measurement and relationship to gender and specialty. Am J Psychiatry. 2002;159(9):1563-9.
- [Google Scholar]
- The Jefferson Scale of Physician Empathy; Development and preliminary psychometric data. Educ Psychol Meas. 2001;61(2):349-65.
- [Google Scholar]
- Personality and performance correlates of empathic understanding in psychotherapy In: Tomlinson T, Hart J, eds. New directions in client centered therapy. Boston: Houghton-Mifflin; 1968.
- [Google Scholar]
- Correlates of empathy in psychotherapy: a replication. J Abnormal Psychology. 1969;74(4):477-81.
- [Google Scholar]
- How do distress and well-being relate to medical student empathy? A multi centered study. J Gen Intern Med. 2007;22(2):177-83.
- [Google Scholar]
- Sex differences in empathy and related capacities. Psychol. Bull. 1983;94(1):100-131.
- [Google Scholar]
- An empirical study of decline in empathy in medical school. J Med Edu. 2004;38:934-1.
- [Google Scholar]
- An analysis of empathy in medical students before and following clinical experience. J Med Edu. 1981;56:1004-10.
- [Google Scholar]
- Administrator's Manual for the sixteen personality factor questionnaire. Illinois: IPATInc; 1972.
- [Google Scholar]
- A New Scale of Social Desirability Independent of Psychopathology. Journal of Consulting Psychology. 1960;24(4):343-354.
- [Google Scholar]
- An analysis of empathy in medical comparisons of nurses and physicians on an operational measure of empathy. Evaluation and the Health Professions. 2004;27(1):80-94.
- [Google Scholar]
- Emotional intelligence and the identification of emotion. Intelligence. 1996;22(2):89-114.
- [Google Scholar]
- World Health Organization. Geneva. 2000. 2000. [web page on the Internet]. Available from www.who.int/mentalhealth/media/en/62.pdf Accessed March 8 2008
- [Google Scholar]
- Psychological Theories. [web page on the internet]. Available from www.http://law.jrank.org/pages/809/Crime-Causation-Psychological-Theories-Individual-influences.html Accessed March 8 2008
- [Google Scholar]
- Accessed March 8 2008www.http://eqi.org/empathy.htm
- Psychological test taking anxiety and response style indices during aircrew medical evaluation. MD Dissertation, Rajiv Gandhi University of Health Sciences, Bangalore.
- [Google Scholar]
- Test taking response styles and associated personality traits in aircrew during medical evaluation. Indian Journal of Aerospace Medicine. 2005;49(2):1-10.
- [Google Scholar]
- How do physicians teach empathy in the primary care setting? Acad Med. 2002;77(4):323-28.
- [Google Scholar]




