
Translate this page into:
Non-specific tinnitus in a helicopter pilot: Aeromedical perspective


*Corresponding author: R. Preethi, Resident in Aerospace Medicine, Institute of Aerospace Medicine, Bengaluru, Karnataka, India. preethiofficial05@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Preethi R, Sekhar MB, Fatima SS, Ghosh G. Non-specific tinnitus in a helicopter pilot: Aeromedical perspective. Indian J Aerosp Med 2024;68:67-70. doi: 10.25259/IJASM_24_2024
Abstract
Tinnitus is the perception of noise in the absence of any external sounds. High intensity noise exposure of aircrew increases the incidents of hearing loss and tinnitus. It can be associated with hyperacusis or hearing loss. Tinnitus may interfere with the cockpit communication and have flight safety implications. This paper presents a case of a military helicopter aircrew having non-specific tinnitus with emphasis on aeromedical assessment & disposal. The case is of a 52-year-old male helicopter pilot, who is a known case of primary hypertension (on medication) and pre-diabetes developed bilateral progressive tinnitus. His magnetic resonance imaging brain, serial pure tone audiometry and brainstem evoked response audiometry (BERA) showed normal reports. He was gradually upgraded to unrestricted flying category after sufficient ground observation and aeromedical evaluation. Though there is significant prevalence of tinnitus in aircrew, a standard guideline for evaluation & disposal have not been described in any military/civil aeromedical literatures. This paper aims to discuss about aeromedical concerns & a proposed guideline for evaluation & disposal of tinnitus. Objective assessment of tinnitus, psychological assessment and rehabilitation holds significant relevance in aeromedical disposal of a case of tinnitus in an aircrew. Specific guidelines and policies may be formulated for implementation of the same.
Keywords
Non-specific tinnitus
aircrew
tinnitus matching
aeromedical guidelines
tinnitus

INTRODUCTION
Tinnitus is an acoustic sensation perceived by a person which is not produced by any external source. This can be an intermittent or continuous sensation. Tinnitus can be classified into two types – subjective tinnitus, which is heard only by the patient and objective tinnitus which can be appreciated by the medical examiner as well.[1]
It has a wide range of etiological factors. Subjective tinnitus can be due to otologic causes such as otitis media, Meniere’s disease, impacted wax or noise induced hearing loss, metabolic causes such as thyroid abnormalities, obesity or hyperlipidemia, neurological causes such as head injury, multiple sclerosis, brain hemorrhage or cardiovascular diseases such as hypertension or anemia, ototoxic drugs or psychogenic causes. Causes of objective tinnitus include congenital arteriovenous malformations, glomus tumor, carotid artery aneurysm or stenosis, patulous eustachian tube, or palatal myoclonus.[2]
Although there are a large number of theories explaining the pathogenesis of tinnitus theory of spontaneous otoacoustic emissions (spontaneous otoacoustic emissions generated by electrical activity of outer hair cells), discordant theory (discordant dysfunction of damaged outer hair cells) and edge theory are the most accepted ones.[3] Proper guidance on evaluation and disposal of tinnitus in military or civil aircrew are seldom discussed in aeromedical protocols available worldwide. This article brings out aeromedical considerations and a proposed guideline for evaluation and disposal of a case of tinnitus in a military helicopter pilot.
CASE REPORT
A 52-year-old military helicopter aircrew, with total 4010 h of flying experience, is a known case of systemic hypertension on medication (Tab Telmisartan and Tab Amlodipine) for past 9 years and prediabetes. The aircrew had insidious onset of ringing sensation in both the ears lasted for 1 year duration which was initially occasional and later progressed to continuous in nature and was associated with mild headache. His pure-tone audiometry (PTA), tympanometry, BERA, magnetic resonance imaging brain and cerebellopontine (CP) angle, and neurovestibular evaluation results were within normal limits.
He was diagnosed as a case of normal hearing with no obvious pathology and non-specific tinnitus. He was initially placed in restricted flying category for 12 weeks for observation of the progression of disease if any followed by which he was advised an in-flight evaluation for effectiveness of radiotelephonic (R/T) communication in the presence of aircraft noise and vibration during different phases of the sortie. After a satisfactory performance in the in-flight evaluation and considering his normal hearing status, he was assessed fit for unrestricted flying. His tinnitus was reported to be suppressed in the presence of background noise of sorties and he never presented with any psychological manifestations of tinnitus. Although he remained symptomatic during his subsequent follow-up reviews, he continued in unrestricted flying status considering the normal hearing status and complimentary in-flight test report.
DISCUSSION
Exposure to high intensity noise in combat areas and aviation environment can lead to high frequency hearing loss and tinnitus.[4] Complaints of tinnitus are relatively common among aircrew and can create impairment in their sensitivity to noise, interfere with cockpit communication and distractions in their duty.[5] Therefore, extensive mitigation of risk factors and causes and evaluation on functional performance of the aircrew is very important in an aircrew with tinnitus.
Age of the person and long duration of exposure to high noise environment could have been major risk factors for tinnitus in this case. However, no investigations were suggestive of any association with hearing loss. Tinnitus patient draws more attention toward auditory input and, hence, causes impairments in executive attention. This can, in turn, lead to problems in speech comprehension in chronic cases, adversely affecting in-flight communications and auditory warning signs especially in difficult listening conditions.[3] Tinnitus itself is a stressor causing functional impairment and it will further lead to psychological stress – this vicious cycle will lead to worsening of performance of the aircrew.
Impairments in attention, concentration, and sleep initiation will get aggravated in quiet environments. The brain dopaminergic pathway and tinnitus perception involve common structures and this could be the possible reason for non-auditory effects of tinnitus such as impairment in short-term memory, learning, motivation, emotions, and mood [Figure 1]. Attentional narrowing for better auditory cues can lead to omissions and errors. Impairment in spatial working memory may affect situational awareness.[6] Lifetime prevalence of depression is significantly increased in patients with tinnitus, implies the importance of psychological evaluation, and it’s significance in flight safety.[7] In this case, systemic hypertension and antihypertensive medication he is on (Amlodipine) can cause tinnitus by damage to cochlear microcirculation.
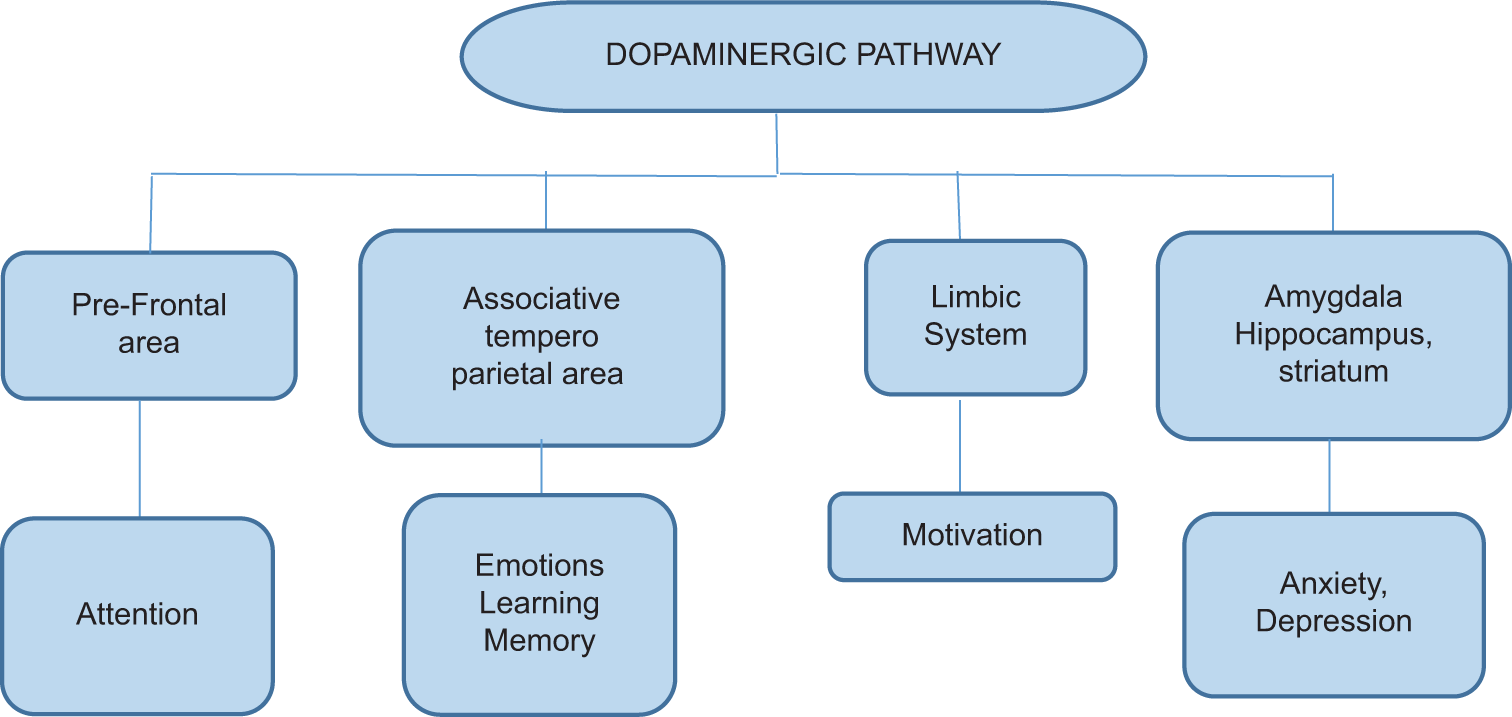
- Non-auditory effects of tinnitus.
There are various methods of subjective assessment of tinnitus – Tinnitus Handicap Inventory, Tinnitus Reaction Questionnaire, etc. Objective assessment methods include PTA, neuro-vestibular assessment, neuro-imaging, and tinnitus matching which gives more reliability to the evaluation. Tinnitus matching identifies and characterizes specific characteristics of a person’s tinnitus using a clinical audiometer. It includes tests such as pitch matching, loudness matching, octave confusion test, minimum masking level, loudness discomfort level, and residual inhibition. It can be used for analysis of severity and management if required.[8] A psychological evaluation to assess any associated sleep or mood disturbances and cognitive decline has to be carried out by an aviation psychologist before further disposal of the cases.
Management of tinnitus includes different components such as reassurance, cognitive behavioral therapy, relaxation and neurofeedback, tinnitus masking (especially during sleep), and tinnitus retraining therapy (TRT) (Habituation of tinnitus and Habituation of Reactions to tinnitus).[9] Hyperbaric oxygen therapy has shown to cause a considerably beneficial effect in treatment of tinnitus, especially in chronic conditions along with simultaneous pharmacotherapy.[10]
Aeromedical disposal of a case of tinnitus in an aircrew is currently based on degree of hearing impairment and none of the existing national or international civil or military guidelines mention any specific criteria for evaluation and disposal of non-specific tinnitus. A case of tinnitus requires extensive evaluation and all the possible causes of tinnitus should be ruled out. Case of secondary tinnitus should be managed based on the clinical scenario. If it is associated with hearing loss, hearing sensitivity and severity should also be considered.
For non-specific tinnitus, aviation psychologist assessment should be done at Institute of Aerospace Medicine, Bengaluru. Tinnitus matching can be done and if indicates need of treatment, TRT and/or psychotherapy and neurofeedback are recommended. During the period of TRT, the patient should be placed in non-flying category for a period of 24 weeks so as to prevent any worsening of the condition during the course of treatment and to accurately analyze the effectiveness TRT. If there is improvement of functional state with the therapy, an on-ground evaluation may be carried out regarding performance on R/T communication before putting the aircrew back to the cockpit. The inherent noise attenuation properties of the aircrew helmet can adversely affect the symptoms as tinnitus has tendency to worsen when in quiet environment which should also be considered during on ground assessment. If the assessment is complimentary, aircrew can be reviewed for possible upgradation to restricted flying category. Further upgradation requires an in-flight evaluation of the aircrew. If successful, aircrew may be awarded unrestricted flying category with annual follow-up by an ENT specialist locally so as to detect any worsening of the symptoms at the earliest [Figure 2].
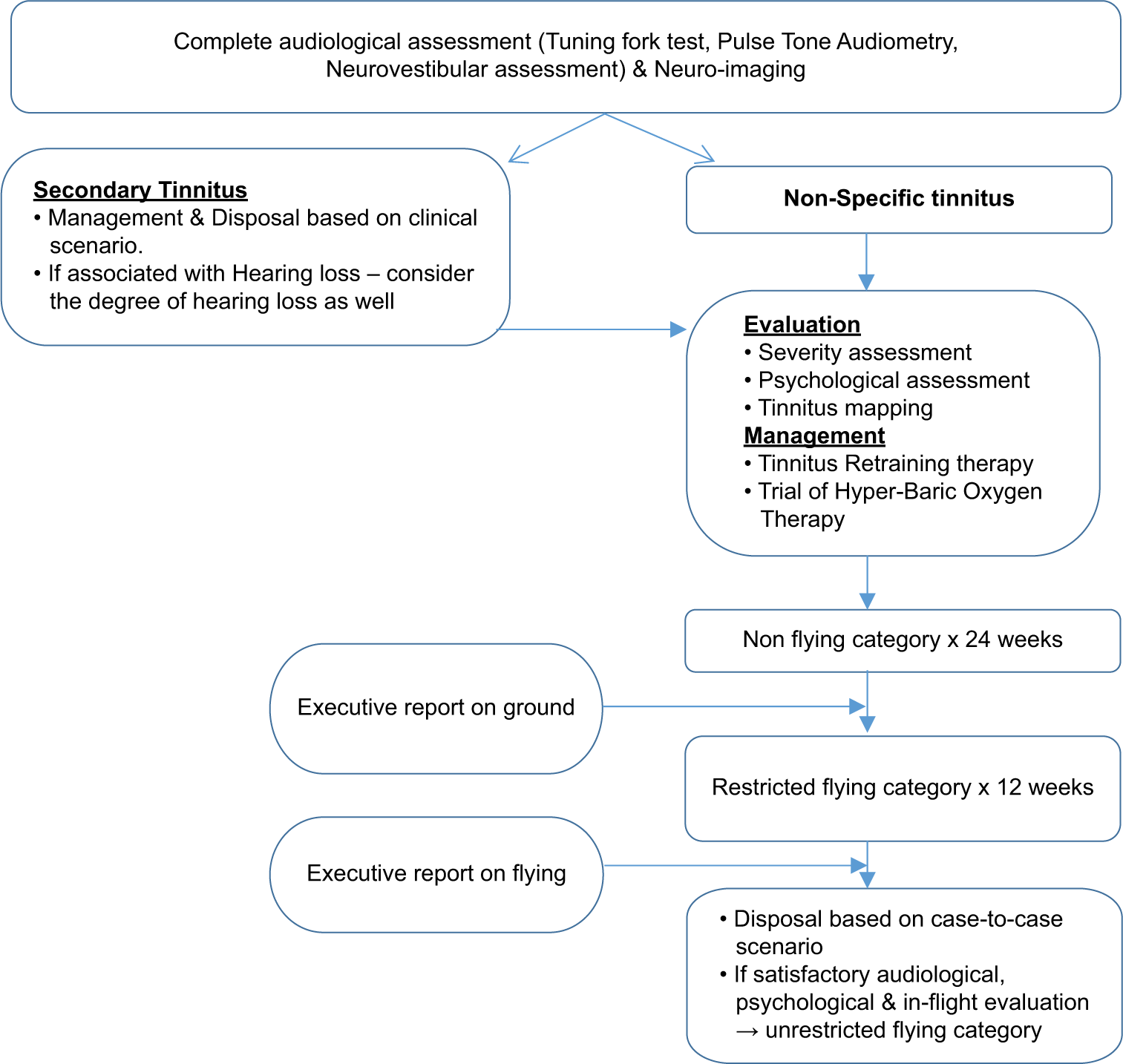
- Aeromedical evaluation and disposal of a case of tinnitus.
CONCLUSION
Objective assessment of tinnitus, psychological assessment and rehabilitation holds significant relevance in aeromedical disposal of a case of tinnitus in an aircrew. Specific guidelines and policies may be formulated for implementation of the same.
Acknowledgment
The authors would like to express their sincere gratefulness to Dr. Binu Sekhar M, Indian Air Force, for scientific advice for the completion of this article. We are also grateful to Dr. S S Fatima, Indian Air Force, and Mr. Gaurab Ghosh for the encouragement and contribution towards the scientific discussion on the disposal of the case. We would also like to express our humble gratitude to the subject for his forbearance and sincerity in sharing adequate details.
Ethical approval
The Institutional Review Board has waived the ethical approval for this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Tinnitus: Clinical experience of the psychosomatic connection. Neuropsychiatr Dis Treat. 2014;10:267-75.
- [CrossRef] [PubMed] [Google Scholar]
- Tinnitus: Characteristics, causes, mechanisms, and treatments. J Clin Neurol. 2009;5:11-9.
- [CrossRef] [PubMed] [Google Scholar]
- Noise-induced hearing loss and tinnitus in military personnel. Mathews J Emerg Med. 2017;2:27.
- [Google Scholar]
- Tinnitus among airline pilots: Prevalence and effects of age, flight experience, and other noise. Aviat Space Environ Med. 2009;80:112-6.
- [CrossRef] [PubMed] [Google Scholar]
- Chronic tinnitus: Association with psychiatric diagnoses. J Psychosom Res. 1987;31:613-21.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of tinnitus complaints and probable association with hearing loss, diabetes mellitus and hypertension in elderly. Codas. 2013;25:176-80.
- [CrossRef] [PubMed] [Google Scholar]
- Tinnitus dopaminergic pathway. Ear noises treatment by dopamine modulation. Med Hypotheses. 2005;65:349-52.
- [CrossRef] [PubMed] [Google Scholar]
- Appendix II. Guidelines for recommended procedures in tinnitus testing In: CIBA foundation symposium. Vol 85. CIBA; 1981. p. :303-6.
- [CrossRef] [Google Scholar]
- Usefulness of hyperbaric oxygen therapy in patients with sensorineural acute and chronic tinnitus In: International Congress Series. Vol 1240. Netherlands: Elsevier; 2003. p. :277-86.
- [CrossRef] [Google Scholar]




