Translate this page into:
3D-Cardiovascular cartography: A novel non-invasive technique for coronary screening in aircrew
Abstract
Cardiovascular screening to exclude coronary artery disease (CAD) forms a very important part of any aircrew evaluation. A routine ECG forms part of initial evaluation for aircrew duties. As the incidence of CAD is age related, repeat ECG examination and even periodic Bruce protocol stress test are mandatory requirements by certain Regulatory Agencies including India. Routine use of cardiac stress testing has been controversial because of inadequate specificity when applied to an asymptomatic population. At times further invasive tests for delineation of the coronary arteries become necessary for the apparently normal aircrew. Availability of population health data and increasing use of computer applications in medical database management have made risk analysis and risk stratification easier and more reliable. This paper discusses the use of a truly non-invasive protocol for routine coronary screening, especially of aircrew. The first part of the protocol involves the use of a simple computer - based algorithm developed using the Framingham study with various risk factors including age, gender, family history, smoking habit, body mass index, blood pressure, cholesterol and HDL levels. The software predicts the coronary risk of the individual based on population data. The second part of the protocol involves the use of a novel new technique of 3-D Cardiovascular Cartography (CCG). This is based on 3-D mathematical modeling and simulation using high speed computation enabling non-linear hemodynamic to be evaluated from beat-to-beat recording of the cardiac cycle. The regional coronary circulation is calculated. It is recommended that the scope of using these non-invasive methods in routine cardiovascular evaluation of the aircrew be considered. The data obtained by these techniques will also be useful in aircrew maintenance programmes based on preventive cardiology.
Keywords
Coronary artery disease
ECG examination
cardiovascular cartography
Coronary circulation

Flying an aero plane is an occupation that demands repeated successful demonstration of a minimum standard of physical and mental fitness by its operator. The objective of the regulatory authority will always be to rule out even the remotest possibility of a sudden incapacitation of the pilot while at the controls. The medical regulations thus insist on clauses to preclude such events as epilepsy, incapacitating angina, altered consciousness or sudden death.
Cardiovascular screening
Cardiovascular screening to exclude CAD thus forms a very important part of any aircrew evaluation. A routine ECG forms part of initial evaluation for aircrew duties. As the incidence of CAD is age-related, repeat ECG examination and even periodic Bruce protocol stress test are mandatory requirements by certain regulatory agencies including India[l]. The following are some of the important considerations in this respect :
The resting ECG is an insensitive tool for the detection of presymptomatic CAD although it identifies a small number who have suffered a silent myocardial infarction [2].
The risk of sudden death from an unheralded heart attack increases with age. Thus, when compared to a man of 30 years, the risk of sudden death from acute MI increases 8 times at 40 years, 36 times at 50 years and 100 times at 60 years. Further, 50% of those dying suddenly do so without premonitory symptoms [3].
Sudden death is the initial presentation in more than one third of MI with up to 60% of patients dying in the first hour. Other initial symptoms may include incapacitating angina or altered consciousness, both equally dangerous when occurring inside the cockpit environment.
Aero medical stresses such as heat, hypoxia, hyperventilation and high- +Gz manoeuvres may provoke dysrhythmia or infarction in individuals with pre-existing coronary artery lesions [4].
Exercise ECG is not a routine mandatory requirement for aircrew evaluation neither in the ICAO ISARPs [5] nor in the JAR [6]. The predictive value of an abnormal treadmill test for significant CAD in men average about 21%, with values ranging from 5% to 46%, but in most studies were less than 25% [7]. The poor yield of exercise testing due to the relatively low prevalence of CAD in the healthy aviator population must be recognized. While there is general agreement that CAD is a disqualification in the context of military aviation, careful consideration supported by detailed evaluation is made mandatory in the case of civil aircrew. Regulatory authorities may often take the easy option of denying licenses to civil aircrew detected to have CAD on routine testing. The Federal Aviation Authority (FA A) has an exceptional record of granting medical waivers to pilots with evidence of CAD following painstaking evaluation as can be seen from the figures in Table 1.
| Event | Type of License | ||
|---|---|---|---|
| Class I | Class II | Class ffl | |
| Myocardial infarction | 299 | 323 | 2,819 |
| Percutaneous trans- | |||
| luminal angioplasty | 354 | 278 | 2233 |
| One or more | |||
| coronary stents in thesame time frame | 213 | 173 | 1,289 |
| Coronary artery bypassgrafting | 256 | 295 | 3,197 |
| Atherectomy | 51 | 10 | 227 |
Some of the newer tests for coronary evaluation, though not yet widely available, include the following:
Imaging for coronary artery calcification
Stress radionuclide imaging
Stress echocardiography
Non-invasive coronary angiography, such as electron beam computed tomography (EBCT), magnetic resonance angiography (MRA)
Coronary angiography is the 'gold test' which forms the basis for evaluating whether a lesion is non-significant or significant depending on the degree of occlusion of any coronary artery as indicated in Table 2.
| Degree of severity | Occlusion in any coronary artery | Aggregate of occlusion |
|---|---|---|
| Minimal Coronary Artery Disease (MCAD) | < 40% | < 120% |
| Significant Coronary Artery Disease (SCAD) | > 40% | > 120% |
The prevalence of CAD in asymptomatic military pilots is reported to be extremely low even though published figures are not available for India. Among the commercial aircrew and private pilots, this prevalence may be closer to that of the general population. With the treadmill stress test being made mandatory among Indian civil aircrew above the age of 35 years since over 6 years now, a huge database must be available. Its detailed analysis with a view to review the practice will give valuable inputs to regulatory authorities. An abnormal treadmill test continues to generate a lot of anxiety among the aircrew and many physicians are unhappy to subject them to further invasive procedures knowing that the predictive significance of the positive treadmill test in an unselected aviator population may be less than 10% for angiographic significant CAD [8]. Further, as the treadmill tests are being done outside the direct supervision of the physicians of the medical evaluation centers, this policy needs to be reviewed to ensure standardization of the aircrew evaluation procedures.
Coronary Risk Stratification
A suggestion gaining increasing acceptance internationally is the need for risk stratifying the aviator population prior to performing screening tests in order to improve their predictive value.
The authors propose that this suggestion be accepted at the earliest and recommend the following procedures:
History, physical examination, laboratory investigations, etc is utilized to assess the classical CAD risk factors.
Use of simple computer-based risk calculators is used to assess the risk factors quickly and effectively. An example of such an approach will be the use of a Framingham risk index.
If the risk index is above the specified threshold, a graded exercise test may be conducted which will show a better predictive value.
It the stress test is positive, other tests including coronary angiography can be conducted to establish the diagnosis.
Cardiovascular Cartography (CCG)
A novel technique of 3-D (CCG) has recently been developed by Indian scientists. This is based on 3-D mathematical modeling and simulation using high speed computation enabling non-linear hemodynamic to be evaluated from beat to beat recording of the cardiac cycle [9].
As far as the patient and the doctor are concerned the technique is as simple as recording an ECG but with a little more elaborate and precise preparation of the patient. The equipment (Fig 1) uses a vertical acceleration detector that picks up subsonic waves that are transmitted from the heart to the chest wall throughout the cardiac cycle. The recordings of 1024 heart beats include beat to beat stroke volume, systolic time intervals, flow turbulence and arterial blood pressure. Using semodynamic behavior difference is distributed on the predictive model. The resultant deviation specialized digital signal processing and neural network computing, a predictive model of the individual is created and the measured hemodynamic behavior difference is distributed on the predictive model. The resultant deviation difference is distributed as pressure zone, volume zone, time zone and flow zone in a clockwise direction on the cardiovascular cartogram (Fig 2).
- Fig. 1.
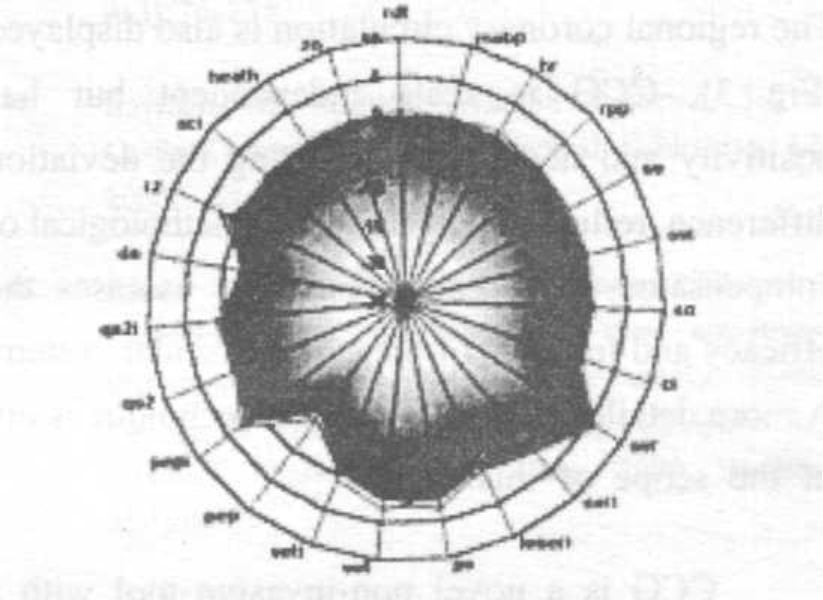
- Cartogram-CAD Negative
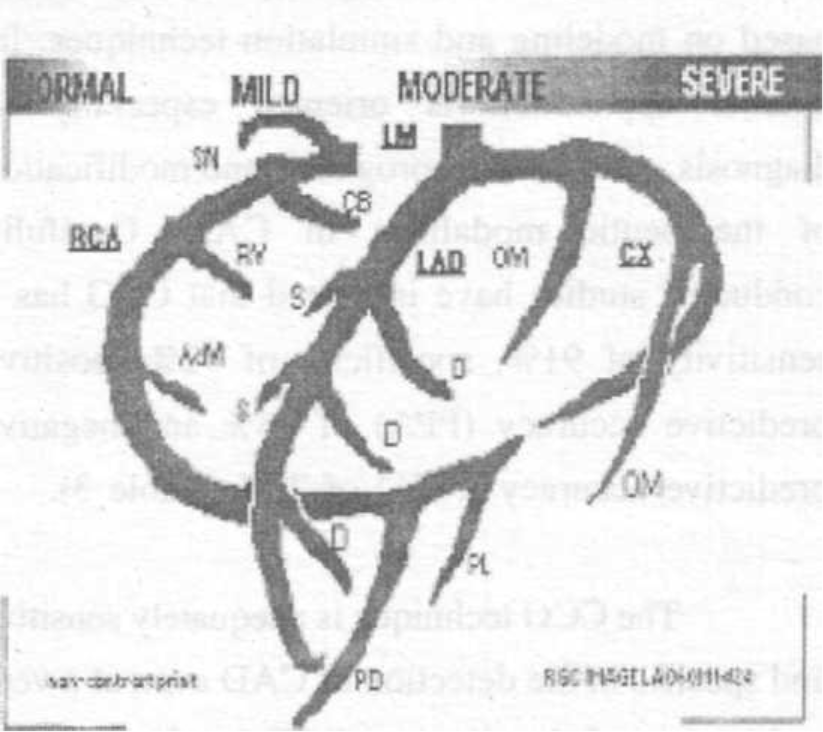
The regional coronary circulation is also displayed (Fig 3). CCG is scale independent but has positivity and negativity indicating the deviation difference, reflecting physiological, pathological or compensatory phenomena and thus assesses the efficacy and function of the cardiovascular system. A more detailed description of the technique is out of the scope of this paper.
- RCG Equipment
CCG is a novel non-invasive tool with a systemic approach for interpreting hemodynamic based on modeling and simulation techniques. Its clinical application is oriented especially to diagnosis, estimation of prognosis and modification of therapeutic modalities in CAD. Carefully conducted studies have indicated that CCG has a sensitivity of 91%, specificity of 92%, positive predictive accuracy (PPA) of 98% and negative predictive accuracy (NPA) of 75% (Table 3).
| Primary presence of CAD | nteroseptal region (LAD) | nferioseptal region (RAC) | ateral region (LCX) | |
|---|---|---|---|---|
| Sensitivity | 91 % | 83 % | 80 % | 72 % |
| Specificity | 92 % | 76 % | 74 % | 80 % |
| PPA | 98 % | 85 % | 80 % | 81 % |
| NPA | 75 % | 74 % | 74 % | 70 % |
| Mean Accuracy | 91 % | 81 % | 78 % | 75 % |
The CCG technique is adequately sensitive and specific in the detection of CAD even at a very early stage of the disease. CCG results compare favorably with other available invasive and non-invasive tests to detect CAD and can be a low cost solution for mass screening of a population for early detection of CAD.
Risk Modification
One of the significant advantages of this combined system of CAD risk stratification followed by noninvasive CCG will be in the field of primary prevention of CAD. As the entire process involves transparent and easy to understand presentations, the subject, viz., aircrew in our context, has total involvement in the evaluation and gets full grasp of the salient features of the underlying mechanisms in the development of CAD. This will help in motivating the aircrew on the preventive measures to improve the clinical risk profile through life style management and other measures.
Conclusion
A novel method of using computer-aided risk analysis and stratification followed by a non-invasive process of CCG is recommended to carry out coronary screening among aircrew. Prompt acceptance of the findings and recommendations on the part of the aircrew will bring about a favorable shift in their attitude towards primary prevention of CAD. Early identification of the risk factors will help in improving their health status with a positive impact on air safety.
References
- Electrocardiographic changes resembling myocardial ischemia in asymptomatic men with normal coronary arteries. British Heart J. 1979;41:14-225.
- [Google Scholar]
- Factors relating to suddenness of death from coronary artery disease: Combined Albany-Framingham studies. Am J Cordial. 1976;37:1073-1078.
- [Google Scholar]
- Clinical Practice Guideline for Coronary Artery Disease, Aerospace Medical Association (Internet)
- [Google Scholar]
- International Civil Aviation Organization: International Standards and Recommended Practices (ISARPs) - Personnel Licensing Annex 1 to the Convention on International Civil Aviation Montreal: ICAO; 1988.
- [Google Scholar]
- JAR-FACL 3: Flight Crew Licensing Medical. Joint Aviation Authorities Hooddorp 1998
- [Google Scholar]
- Guidelines for exercise testing. A report of the American College of Cardiology / American Heart Association task force on assessment of cardiovascular procedures. J Am Coll Cardiol. 1986;8(3):75-738.
- [Google Scholar]
- Clinical Aviation Medicine. (3rd edn). Castle Connolly Graduate Medical Publishing. LLC; :162.
- [Google Scholar]
- Cardiovascular cartography - a new non-invasive technique to detect coronary artery disease. Fourteenth IEEE Symposium on Computer-Based Medical Systems. :26-27.
- [Google Scholar]




