Translate this page into:
Study of Morbidity and Disability Pattern of Civil Aircrew in India: An Analysis of Medical Assessments
Abstract
Introduction:
Analysis of morbidity and disability pattern can provide insight into civil aircrew health issues that could assist in developing preventive and therapeutic intervention programs. This study was carried out to analyse the morbidity pattern among Indian civil aircrew from 2010-2015.
Methodology:
The data for this study was collected from medical assessment records of aircrew (Hard and soft copies) kept at Medical Cell DGCA, India and analysed.
Results:
A total of 274 cases during initial and 95 during renewal medical examination were made permanently unfit. In initial medicals, Ophthalmic diseases (n=103, 37.59%) were the main cause for permanent unfitness. Lattice Degeneration and defective colour perception were the leading diseases. In renewal medicals, Cardiac diseases (n=20, 21.05%) and Orthopaedic conditions (n=20, 21.05%) were the main causes for permanent rejection. In Cardiac group, and as an overall cause of disability, CAD (n=16, 16.84%) was the leading diagnosis for permanent rejection in renewal medicals. Age wise data analysis reveals that younger age group pilots are getting permanently rejected because of eye diseases (n=97, 35.01%) and older age group crew because of cardiac causes. Year wise data analysis for initial medicals revealed that, Eye diseases are still contributing maximally to rejection in initial medicals, but other medical conditions and cardiac diseases are showing an increasing trend. Eye and ENT diseases are showing rising trend in year 2015 for permanent rejection in renewal medicals.
Conclusions:
The main purpose of medical examination is to identify disabilities that may affect flight safety. The possible reasons for existing morbidity trends among commercial aircrew are discussed along with Implications for preventive and therapeutic strategies.
Keywords
Civil aircrew
DGCA
Initial medical examination
Renewal medical examination

Introduction
Civil Aviation Industry has progressed tremendously in past few years in India, which has caused an increase in the number of individuals taking up flying as their career of choice. The aircraft environment differs from other occupational environments in terms of aviation stresses, which necessitates maintenance of high standards of physical and mental health in aircrew. Civil aircrew are comprehensively examined initially before issue of any flying licence and then at periodic intervals to monitor their health issues. This system of periodic medical examination helps in detecting any disease which can compromise flying fitness of an aviator and eventually result in a catastrophe. Hence regular health examination is an important link in maintaining flight safety. The general medical requirements for civil aircrew are governed vide Chapter 6 of Annex 1, ICAO Manual of Civil Aviation Medicine and Civil Aviation Requirements of DGCA (CAR)[1].
Rejection for flying duties on account of any illness results in loss of skilled man power and is detrimental to a pilot in terms of career progression and has financial implications. Hence knowledge of disability and morbidity patterns affecting aircrew is important to update medical policies or form new ones.
To identify the common ailments that lead to permanent unfitness, a comprehensive analysis of available data was undertaken with an aim to determine morbidity and disability pattern in commercial aircrew in India.
Material and Methods
The data for this study was collected from medical assessment records of aircrew kept at Medical Cell DGCA. This data consisted of assessment records of initial and renewal medical examination in respect to Cl-I and II medicals. The source of data was hard copies of CA-35 and medical assessments in respect to permanent unfit cases, which were issued to aviators from 2010 to 2015. The available data was collected under the heads of Age, Sex, Year of evaluation, Type of licence, Type of Disease and Type of medical examination.
Analysis of Data
The data was analysed separately for initial and renewal medical examinations. The data pertaining to different diseases was grouped into major disease groups like Cardiac, ENT, Eye, Neurological, Orthopaedics, Surgical, Other Medical conditions etc. The most frequent group of diseases causing permanent disabilities was identified. Common diseases were identified in each group that contributed maximum to morbidity. The data was also analysed in terms of age and gender vis a vis types of disabilities. Year wise changing trends of diseases causing permanent unfitness was also analysed.
Results
As per DGCA records, presently there are a total of about 12,000 active pilots in India. Approximately 18,000 medical assessments are conducted annually for civil aircrew in India which includes CL-I and II types of medicals for different types of licenses.
Permanent Unfit Cases During the study period from Jan 2010 to Dec 2015, a total of 369 civil aircrew were detected to be permanently unfit. Out of these 326 were males and 43 females. During initial medicals, 241 males and 33 females were made permanently unfit. In the renewal medicals, 85 males and 10 females were declared permanently unfit (Fig 1).
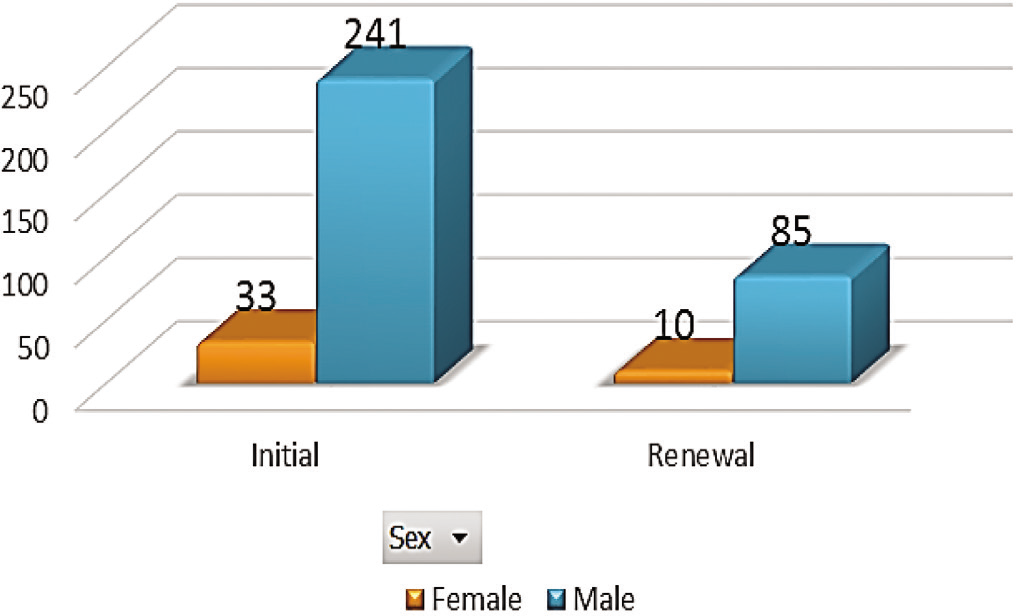
- Gender distribution for permanent unfit cases in initial and renewal medicals
Analysis of Permanent unfit cases in Initial Medical Examinations
In the initial medicals in males, Ophthalmic diseases were the main group, followed by ENT group (Fig 2). For females, during Initial medicals Neurological disabilities (mainly abnormal EEG) formed the majority group, followed by ophthalmic diseases.

- Gender wise disease groups for permanent unfit cases in initial medical examination
As shown in Table 1, overall, in initial medicals, Ophthalmic diseases (n=103, 37.59%) were the main cause for permanent unfitness. Lattice Degeneration and Defective Colour Perception were the leading diseases. Large number of aircrew were declared unfit because of Neurological causes also (n=40, 14.59%), in which abnormal EEG was the most common diagnosis. In ENT group, substandard hearing (n=9) was the leading cause of disability. In Cardiac group, Hypertension (n=10) caused maximum permanent rejections, affecting younger age group also. In surgical group, Renal calculus (n=12) caused maximum rejections.
| Age | Cardiac | ENT | Eye | Neuro | ObsGynea | Other Medical | Surgical | Uncategorised | Ortho | Grand Total |
|---|---|---|---|---|---|---|---|---|---|---|
| < 20 | 7 | 6 | 28 | 8 | 2 | 4 | 2 | 1 | 58 | |
| 21 - 30 | 19 | 29 | 69 | 30 | 1 | 14 | 27 | 7 | 196 | |
| 31 - 40 | 3 | 1 | 4 | 8 | ||||||
| 41 - 50 | 1 | 1 | ||||||||
| 51 - 60 | 5 | 2 | 1 | 1 | 9 | |||||
| > 60 | 1 | 1 | 2 | |||||||
| Grand Total | 31 | 36 | 103 | 40 | 1 | 21 | 32 | 9 | 1 | 274 |
Analysis of Permanent unfit Cases in Renewal Medical Examinations
In the renewal medicals in males, Cardiac diseases (n=20, 23.52%) were the main group, followed by Ophthalmic diseases (n=15, 17.64%) (Fig 3). For females, Other Medical diseases formed the majority group (n=4,40%) (fig 2).
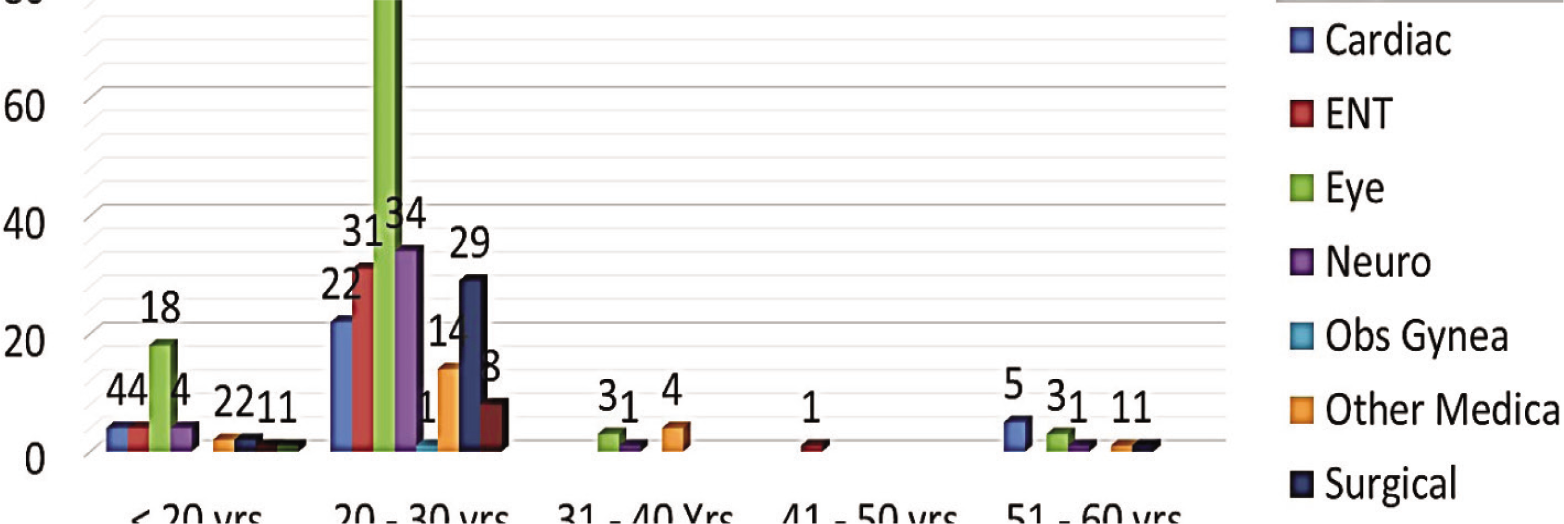
- Initial Medicals : Age wise distribution of disease groups
As shown in Table 2, in renewal medicals, overall, Cardiac diseases (n=20, 21.05%) and Other Medical disease group (n=20, 21.05%) were the main causes for permanent rejection. In Cardiac group, and as an overall cause of disability, CAD (n=16, 16.84%) was the leading cause for permanent rejection.
| Age | Cardiac | ENT | Eye | Neuro | Other Medical | Surgical | Uncategorised | Ortho | Grand Total |
|---|---|---|---|---|---|---|---|---|---|
| 20 - 30 Yrs | 1 | 5 | 2 | 1 | 1 | 3 | 1 | 14 | |
| 31 - 40 Yrs | 1 | 3 | 1 | 5 | 3 | 1 | 1 | 15 | |
| 41 - 50 yrs | 2 | 3 | 2 | 5 | 2 | 1 | 15 | ||
| 51 - 60 yrs | 12 | 3 | 4 | 8 | 5 | 1 | 3 | 36 | |
| > 60 yrs | 6 | 2 | 2 | 1 | 3 | 1 | 15 | ||
| Grand Total | 20 | 4 | 16 | 9 | 20 | 14 | 7 | 5 | 95 |
Effect of Age on Medical Disability
Fig 3 reveals that, in initial medicals, younger age group pilots ( < 30 yrs) are getting rejected because of eye diseases (n=97, 35.01%) and older age group aircrew (>30 yrs) because of cardiac causes.
As shown in Fig 4, in renewal medicals, for younger aircrew (20 – 30 yrs), Eye diseases are the leading cause for unfitness. Other Medical conditions are the major contributing cause for middle age group (30 – 50 yrs). Cardiac conditions are leading cause for rejections in older age group(>50 yrs).
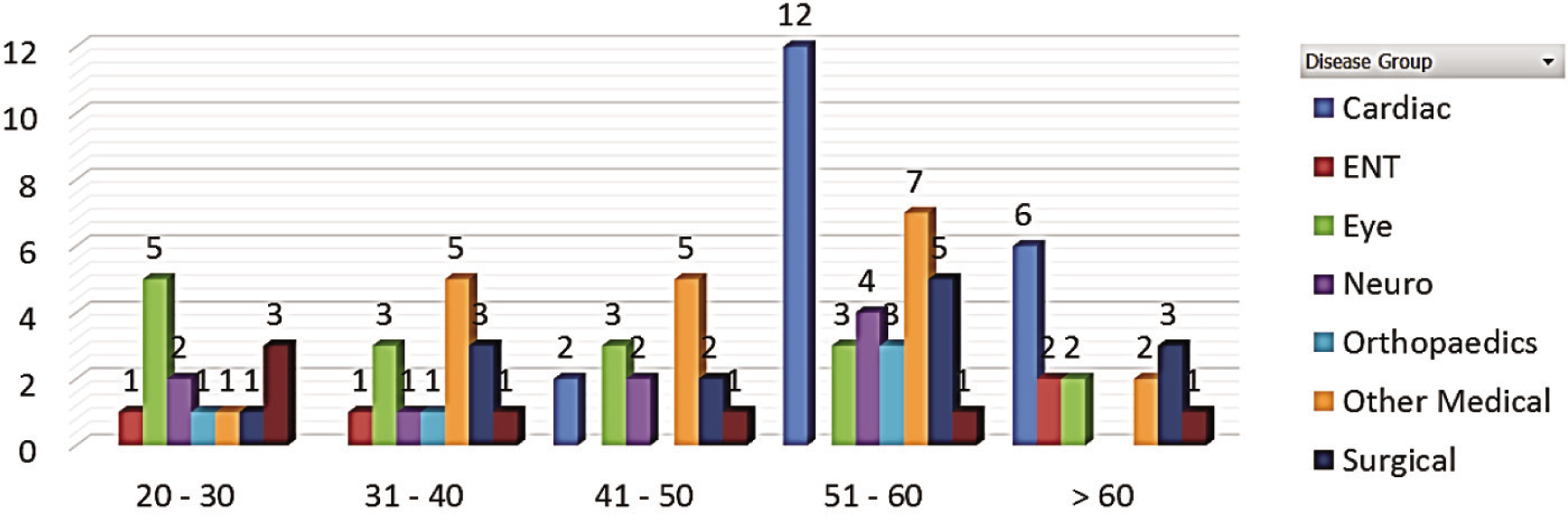
- Renewal Medicals: Age wise distribution of disease groups
Year wise trend of permanent medical disability
As shown in Fig 5, year 2012 witnessed highest number of permanent rejections (n=101), and thereafter the trend shows a decreasing pattern. Since 2013 number of rejections in initial medicals shows a decreasing trend as compared to renewal medicals. In 2015 more candidates got rejected in renewals as compared to initial medicals.

- Year wise distribution of permanent unfit cases in Initial and Renewal medicals
Fig 6 reveals that, Cardiac diseases have a more or less uniform trend over the years and are primarily responsible for permanent rejections during renewal medicals.

- Renewal Medicals: Year wise distribution of disease groups
As shown in Fig 7, Eye diseases contribute the maximum to permanent rejections in initial medicals as compared to other diseases.
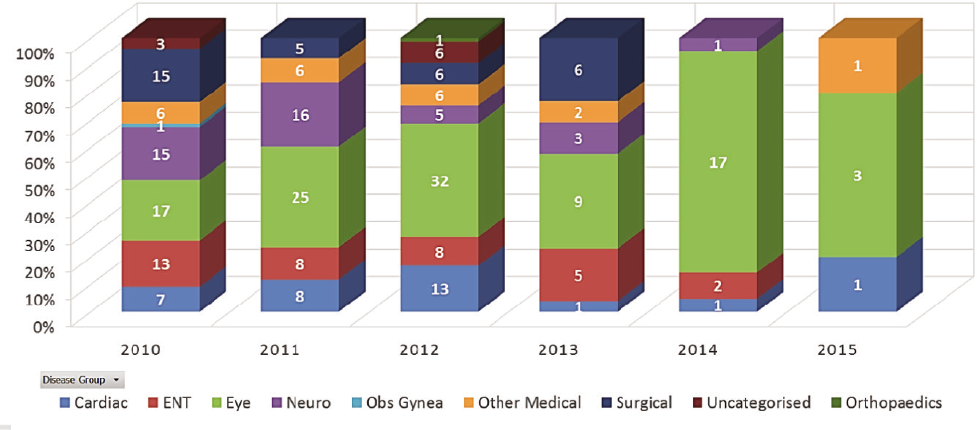
- Initial Medicals: Year wise disease groups distribution
Irrespective of type of medicals, Ophthalmic causes are the maximum contributors to permanent rejections in younger age group and Cardiac diseases for older age group.
Discussion
In India, DGCA under Ministry of Civil Aviation is the regulatory authority for medical standards and fitness of commercial aircrew, the guiding principles being based on ICAO standards. Civil aircrew in India hold different types of licences like SPL, CPL, ALTP etc for which they undergo initial and renewal medical examinations as per laid down guidelines at specific intervals.
There are three types of medical examinations conducted, namely CL-I, II and III depending on type of licence applied for or held;the highest degree of medical standards being envisaged in Cl-I (CPL,CHPL,ALTP etc). Medical assessment record of CL-I and II medicals are maintained at Medical Cell, DGCA.
As per DGCA regulations, an applicant for medical assessment shall undergo a medical examination based on the following requirements:
Physical and Mental
Visual and Colour Perception
Hearing
Keeping in view the aviation stresses and occupational risk associated with flying a commercial aircraft, strict medical examination schedule is followed for civil aircrew for timely detection of any disease having potential to jeopardise flight safety.
With an aim of detecting morbidity and disability pattern among commercial pilots, a study was undertaken to analyse available medical assessment data of last six years at Medical Cell DGCA, which included data on permanent unfit cases from 2010 to 2015. The disabilities in the present study were divided into different groups like Eye, ENT, Surgical, Cardiac, Orthopaedics and Other Medicals (Physical conditions other than Cardiac) for better understanding of distribution of ailments group wise and also individual disease wise.
As brought out in results, total of 369 aircrew were declared permanently unfit during the period of study. Ophthalmic ailments emerged as the single largest group causing permanent rejection in initial medicals wherein Lattice Degeneration (n=30) was the commonest specific Ophthalmic ailment. An earlier study by Wg Cdr P Pant et al. in 2005 [2] also documented disabilities of the eye as one of the major causes of permanent denials at the time of initial medical examination. Majority of these rejections were on account of substandard vision and defective colour perception. In present study also defective colour perception and substandard vision were leading disabilities after Lattice Degeneration. In view of this, aircrew should undergo strict visual examination as per schedule. Year wise disease group distribution (fig 5,6) revealed that Ophthalmic diseases are showing an increasing trend over past years and became the largest group causing permanent rejections in 2015, both during initial and renewal medicals. Medical policy on Ophthalmic disorders have been revised on 13 Jun 16 (AIC 06/2016). As per new policy, Lattice degeneration is no longer a cause for automatic permanent rejection and will be dealt on case to case basis.
In terms of individual disability which caused maximum permanent rejections in initial medicals, EEG abnormality (n=39, 14.2%) ranked first. But after 2013, rejections related to Neuro group and EEG declined as EEG was no more a mandatory investigation for initial Cl-I medicals. This led to decrease in total number of permanent rejections during initial medicals since 2013 (Fig 5).
In the analysis of Cardiovascular disabilities, the point of concern is rise in high blood pressure cases in younger age group, causing permanent unfitness affecting mainly 21 to 30 years’ age group. The previous studies [1,2], did not report this trend. Hypertension in young is an emerging disease in the society and needs to be thoroughly investigated in the younger pilots during medical examinations. Appropriate guidelines are already in place to deal with Hypertension and need to be followed meticulously.
In the analysis of older age group (51 to 65 years) it was found that Cardiovascular ailments are the leading causes for permanent rejection, both in initial and renewal medicals and more so in renewal medical examination (n=18, 18.94%). Earlier studies done in India also reported the same trend [1,2,3]. In the present study, Coronary Artery Disease (CAD) was found to be the commonest disease causing permanent unfitness in older age group both in initial and renewal medicals. Year wise distribution analysis also revealed that Cardiovascular diseases showed similar trend for renewal medicals during the period of study (Fig 6). It highlights the importance of monitoring the cardiovascular status of pilots at regular intervals through present schedule of conducting ECGs, TMTs and other relevant Cardiac investigations.
Earlier studies [4, 5, 6] reported DM-II as one of the leading disability causing permanent rejection [2,3]. In present study DM-II did not show any rising trend. The probable cause may be more awareness in society regarding this disease leading to better control, causing less permanent rejections.
Analysis of surgical group diseases revealed Renal Calculus as the leading disability both in initial and renewal medicals for causing permanent rejection, especially in age group 21 to 30 years (Table 1 and 2). No such observation was made in earlier studies [2,3]. This highlights the importance of USG Abd and KUB, which is done periodically in renewal medicals and should be continued.
There has been a growing demand from aircrew community to increase the renewal medical frequency from 6 monthly to yearly for age group 40 plus, which has recently been agreed to by DGCA. There has been no change in recommended battery of investigations. Looking at the trend of diseases affecting age group 40 years or more, CAD is largely responsible to cause permanent rejections in this group. It may be considered to institute mechanisms like alternate year detailed cardiac and other biochemical investigation or to use predictive tools like the Framingham score and Diabetes Risk Scores to identify higher risk individuals beyond 40 years of age. Nonetheless definitive recommendation cannot be made regarding this issue, based only on data analysis in the present study. An in depth study of temporary unfitness data with emphasis on age wise analysis would be an essential requirement before definite recommendations can be made.
The data for current study was obtained from hard copies of medical assessments, kept at medical cell DGCA. There is a requirement of creating soft copies of these assessments and create a digital data for all these medical assessments. At the time of this study being carried out, efforts were taking shape regarding the same. Digitalization of data is the need of hour for easy storage and accessibility. It will also be useful for analysis and extraction of information whenever deemed necessary like for formulating some new policy.
Conclusions
The main purpose of medical examination is to identify disabilities that may affect flight safety, in time. In the present study, majority of cases were declared permanent unfit due to Ophthalmic disorders in initial medicals as compared to renewal medicals where Cardiovascular disorders were the main cause. Lattice degeneration appeared the most common cause in Ophthalmic group. Revision of AIC for Ophthalmic diseases in Jun 2016 will help in dealing with ophthalmic cases more effectively. Hypertension appeared to cause considerable permanent unfitness even in younger age group. Hypertension in young is an emerging disease in the society and needs to be thoroughly investigated during medical examinations. DM was not identified to be a major cause for permanent unfitness. Investigation profile for age group 40 year plus needs a relook through risk stratification as CAD continues to affect a large number of older aircrew.
Limitations of the Study
9. The data of total number of medicals done in each age group, during initial/renewal medicals and year wise was not available, which restricted further analysis regarding proportional unfitness.
References
- Civil Aviation Requirement (CAR) Section 7 Flight Crew Licensing, Series C, Part-I, Issue 1, 26 August 1999. Rev.2.
- [Google Scholar]
- An analysis of morbidity pattern among civil aircrew. Ind J Aerospace Med. 2005;49(2):24-32.
- [Google Scholar]
- Morbidity pattern in civil aircrew and the medical assessment system for civil aviator in India. Ind J Aerospace Med. 1999;43(2):24-28.
- [Google Scholar]
- Analysis of disability pattern among commercial civil aircrew in India. Ind J Aerospace Med. 1983;27(1):25-29.
- [Google Scholar]




