Translate this page into:
Spondylolisthesis & Spondylolysis
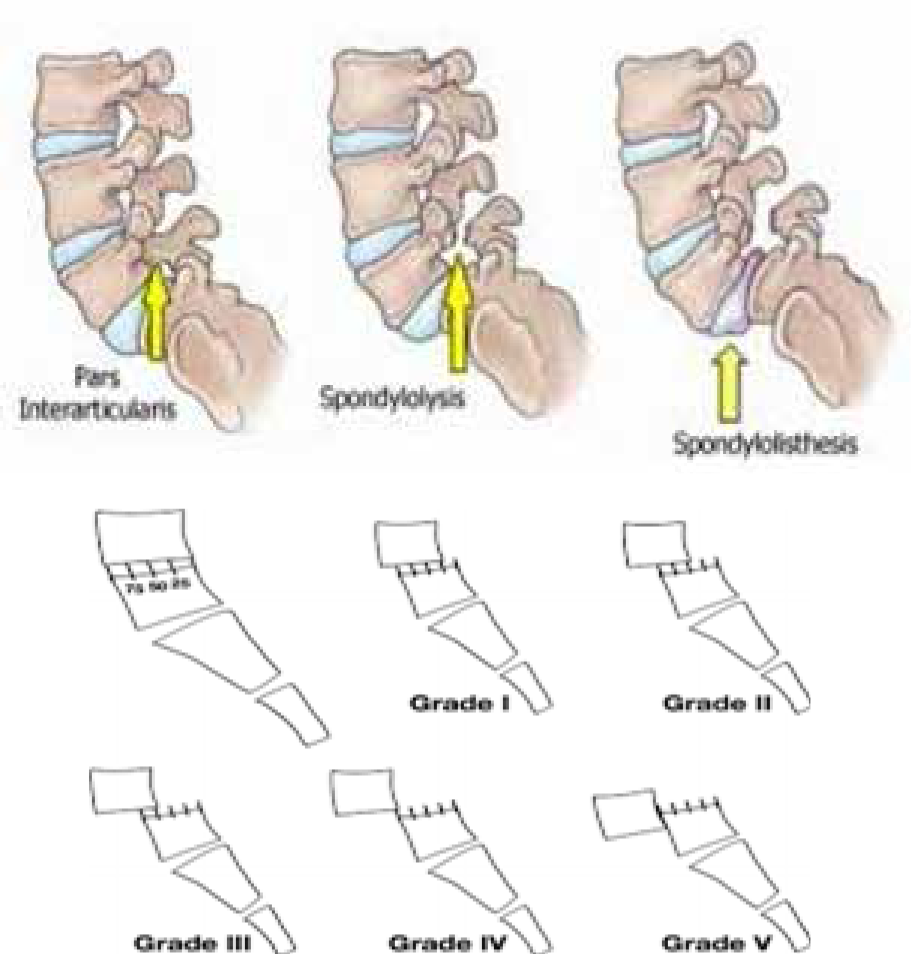
Spondylolisthesis: Spondylolisthesis is a descriptive term used in the slippage or displacement of one vertebra over another [1]. The direction of displacement may be anterior, posterior or laterally. It is commonly associated with Spondylolysis without any neural canal compromise. It is noted in 8% of general population [4].
Causes: The causes can be trauma, pathological fractures due to bone softening diseases like Paget’s disease, Osteogenesis imperfecta, bone tumors, infection of anterior column and degenerative disc disease.
Classification: Many system of classifications are described in the literature but commonly used classifications are dysplastic, Isthmic, degenerative, traumatic and pathologic. The degenerative or closed type due to degenerative or inflammatory disease is commonly seen in older age group. It usually involving L4-5 or L5-S1 vertebrae. The other open or isthmic type seen bilaterally and found in the age group of less than 45 years.
Spondylolysis: The Spondylolysis or break in the pars interarticularis is the descriptive term for defect in superior and inferior articular process of spinal vertebra which is the weakest portion of spinal unit. The deformity is usually bilateral and frequently occur at L5 vertebra. It is seen in 3-7% of population and in early childhood.
Causes: The causes can be unhealed stress fracture due to repeated minor trauma like sports injuries. It may be associated with congenital deformities like spina bifida, wedge shaped vertebrae. The secondary spondylolysis can be seen due to neoplasm, infection and hereditary hypoplasia of pars.
Clinical presentation: The presenting symptoms may be acute or chronic back ache with or without involvement of disc space, neural compression or facetal hypertrophy.
Diagnosis: These deformities can be diagnosed on routine plain radiograph of lumbar spine on lateral radiographic projection [3].The degree of Spondylolisthesis can be graded by fractional shift of one vertebra over the other. In Mayerding Method, the percentage of slippage is graded as Grade I (0-25% displacement), Grade II (26-50% displacement), Grade III (51- 75% displacement), Grade IV (76 -100% displacement) and grade V also known as “spondyloptosis” with more than 100% displacement [2].
Management: Treatment of Spondyolisis & Spondyolisthesis is conservative to start with and consists of bed rest, analgesics and bracing. If conservative treatment is found inefficient, surgical procedures including spinal fusion are the available options. The goal of surgery is to stabilize the segment with listhesis and decompress any neural element under pressure [7]. The spinal fusion surgery is indicated in cases having neurological signs of radiculopathy, slippage of more than 50%, Instability of the segment with progressive listhesis, traumatic or iatrogenic spondylolisthesis, postural and gait abnormality.
Aeromedical concerns: An aircrew suffering from Spondylolysis and or spodylolisthesis will be often symptomatic with low backache and radiculopathy [8]. In addition, continued exposure to vibration and accelerative forces in flight may aggravate the condition of spondylolisthesis by causing further vertebral slippage. The neurogenic claudication due to narrowing of lumbar spinal canal leads to exertional pain radiating to buttocks and thigh on prolonged standing or walking thus adversely affecting performance. Therefore, aircrew requiring regular analgesics to alleviate the pain has to be relived from flying duties.
Aeromedical disposal: Radiological evidence of Spondilolisthesis and Spondylolysis disqualify the candidates for serving in Indian Air Force [9]. However, inservice candidates having these disabilities are assessed for aircrew duties based on functional assessment and neurosurgical opinion. Disposal of the experienced/ trained aircrew depends on the merits of each case based on functional assessment on the restrictions and ability to withstand aviation stress. In the early stages of the disease, utilization of the trained manpower overrides other considerations and revelation of full functional capability without drugs, may justify restricted flying [10]. However, natural progression of the disease and need for medication will probably curtail a long term flying career in most of the cases.
References
- Macnab-I classification of spondyloysis and spondylolisthesis. Clin Orthop Relat Res. 1976;117:23-29.
- [Google Scholar]
- Sondylolisthesis: surgical and treatment results. Surg Gynacol Obstet. 1932;54:371-77.
- [Google Scholar]
- Functional radiography in spondylolisthesis. American Journal of Roentgenology. 2015;204:461-69.
- [Google Scholar]
- Radiographic study of prevalence of spondylolisthesis and LSTV in chronic low back pain subjects. Jorn of Horm Reaseach in Medical and Health Sci. 2014;2(1):12-17.
- [Google Scholar]
- Radiological review Manual (6th ed). North America: Lippincott Williams and Wilkins; 2007.
- [Google Scholar]
- Text book of radiology and imaging Vol II. (7th ed). Edinburgh, Scotland: Churchill Livingstone; 2002.
- [Google Scholar]
- Spondylolisthesis: surgical intervention and treatment results. Surg Gynacol Obstet. 1932;54:371-77.
- [Google Scholar]
- In: Clinical Aviation Medicine. (4th ed). NY: Professional publishing group; 2006. p. :56-57.
- [Google Scholar]
- Section III – Assessment of candidates for flying and ground duty branches and airmen aircrew (Musculoskeletal system and physical capacity) In: IAP 4303 (4th ed). New Delhi: Air headquarters; 2010. p. :95-99.
- [Google Scholar]
- Section VI – Assessment of trained serving personnel (Musculoskeletal system and physical capacity) In: IAP 4303 (4th ed (revised)). New Delhi: Air headquarters; 2016. p. :51-58.
- [Google Scholar]




