Translate this page into:
Rotational field quantum magnetic resonance (RFQMR) in treatment of osteoarthritis of the knee joint
Abstract
Rotational Field Quantum Magnetic Resonance (RFQMR) is a technology that is made to deliver highly complex quantum electromagnetic beams in the sub-radio and near-radio frequency spectrum. The beams can be precisely controlled and focused onto tissues therein generating streaming voltage potentials. In osteoarthritis, this flow in the joint causes forced movement of hydrogen protons in the extra cellular matrix (ECM) due to the alteration in QMR spin in the hydrogen atoms and stimulates the chondrocytes. Thirty-five patients of osteoarthritis were treated with RFQMR focused on both knees for one hour every day for 21 days. They were evaluated before, immediately post treatment and one month after treatment with the Knee Society Scoring System and dynamometry. There was highly significant improvement in Pain Score, Total Knee Score, Total Functional Score, Range of Movement and force of extension, immediately after the treatment vis-a-vis pre treatment values and this improvement persisted when evaluation was repeated after one month. RFQMR is an effective method of treatment of osteoarthritis of the knee joint.
Keywords
Rotational field quantum magnetic resonance
Osteoarthritis

Rotational Field Quantum Magnetic Resonance (RFQMR) beams are delivered by a new computer controlled device called ‘Cytotron’ (Fig 1) that generates precise high intensity Quantum Magnetic Resonance beams from 96 specially designed Mn-Pb-Cu guns (Fig 2) that are focused on a target tissue. It is believed to alter the cell membrane potential in a highly controlled fashion [1,2], Osteoarthritis is a degenerative disease caused by the loss of cartilage from load bearing joints, especially the knees, causing impairment of movement and often severe pain. Many kinds of therapies, including newer drugs have been tried with very little orno success, leaving patients with the only surgical option of joint replacement. This is often beyond the financial reach of patients especially in developing countries [3].
RFQMR Hypothesis in Tissue Regeneration
The study of the interactions between electromagnetic fields and living matter has become a fertile field for research in this century, even though these phenomena have been observed by various civilisations since ancient times. Considerable experimental evidence today points to the possibility of modulating biological functions and structures in a controlled way by inducing electromagnetic (EM) resonance and vice versa, the possibility of detecting and measuring endogenous EM resonance in living organisms and their components as an indicator of biological functions.

- CYTOTRON RFQMR Machine

- Typical QM 60 RFQMR Gum.
There are three types of EM effects on living matter: ionising, thermal and non-thermal effects [4]. Thermal effects induce an increase of entropie disorder in the target, until at certain frequencies and power levels, the effects of ionisation develop. The non-thermal effects are not the result of the transfer of erratic movement by means of an increase of kinetic energy, but rather, in line with the theories of the coherence of condensed matter, they can transmit information that would produce order in the biostructures involved. It is like the tissue response to radio frequency pulse during magnetic resonance imaging. The information content of the quantum EM beams would depend specifically on the waveform, the string of waves, and the time sequence of their modulation. In fact, specific variations in the configuration and temporal exposure patterns of extremely weak EM fields can produce highly specific biological responses, similar to pharmaceutical products [5]. These non-thermal effects are attracting considerable scientific interest mainly because a quantum EM beam is easily modulated and thus is an excellent means for the transmission of information. Studies carried out by various authors suggest the possibility of utilising non-thermal effects even in causing electroporation of the cell membrane [6,7,8,9] to therapeutic advantage.
RFQMR is a technology that is made to deliver highly complex quantum electromagnetic beam pattern in the sub-radio and near-radio frequency spectrum, with precise external command and control.
Based on these studies, it is reasonable to consider patterns in living matter that take into account the EM components of biological structures. Every cell, for instance, is made up of biological and chemical components that can be described in progressively simpler terms down to the elementary molecular constituents of the cells. The cell itself and its internal and external interactions can also be considered in terms of electric and electromagnetic interactions and relationships [10,11,12,13]. Numerous experimental works have shown the possibility of modifying and controlling the selective permeability of the cell membrane by transmitting specialised quantum EM beams. This leads to the possibility of verifying the specific reactions of healthy cells vis-a-vis the reactions of pathological cells and subsequently selecting target cells for therapeutic intervention. Pathological cells are different from healthy cells due to a different tissue composition.
Various authors have reported the modulation of some cell functions, from ionic membrane pumps to many cytoplasmic enzyme reactions, including those connected with cell replication. From these studies it has been seen that the desired effects can be obtained from non-ionising non-thermal RFQMR beams.
Like other tissues, bone and cartilage are constantly being built up and broken down by a variety of metabolic and physical influences. The major stimulus for bone and cartilage formation is a piezoelectric signal generated when these structures are subjected to tension or compression [14,15]. This explains why bone atrophies in the absence of any significant pressure, like weightlessness during space travel or immobilization in a cast.
The transmission of this signal is also impaired following joint injury due to trauma or diseases such as osteoarthritis [16]. RFQMR is designed to characterise and reproduce the piezoelectric signal by altering membrane potential of chondrocytes. This initiates regenerative activities by the induction of a spin in the hydrogen atoms and creates a streaming potential in the extracellular matrix (ECM) similar to that, when bone or cartilage are placed under a load.
In other words, when one takes a step, putting weight on the joint, it compresses the cartilage and thereby displaces the fluid, carrying with it mobile ions, sodium ions and leaves behind the negatively charged proteoglycan carboxyl and sulfate ions. This generates an electric potential due to deneutralisation of negative charges. This is called a Streaming Potential [17].
RFQMR can recreate this Streaming Potential and its restorative rewards in joints impaired due to disease or trauma even though they are at rest. The mechanism of producing this Streaming Potential during resting, natural regeneration while loading and RFQMR induced regeneration of cartilage can be simply put as follows:
At rest. No change in equilibrium between hydrogen protons and negative charge carriers in the extracellular cartilage matrix. Therefore no Streaming Potential, no regeneration at rest.
Natural regeneration. A Streaming Potential is created in the ECM during load bearing caused by the efflux of fixed negative charged fluid forced out of cartilage tissue with active influx of hydrogen protons.
RFQMR induced regeneration. Generation of streaming voltage potential flow in the joint is caused by forced movement of hydrogen protons in the ECM due to the alteration in QMR spin in the hydrogen atoms, causing stimulation of chondrocytes in the ECM.
The present study embodies the results of a new successful and relatively inexpensive treatment of osteoarthritis by the application of Rotational Field Quantum Magnetic Resonance (RFQMR) simultaneously to both knees.
Material and Methods
Thirty-five random subjects, with radiologically severe osteoarthritis were recruited for the study. The condition of their knee joints was first assessed by X-Ray and ultrasound examination at the Department of Radiology, Institute of Aerospace Medicine (IAM), Indian Air Force (IAF), Bangalore. Physical parameters such as height, weight, thigh girth, length of tibia, alignment and stability, goniometrie and dynamometric measurements were carried out at the Department of Human Engineering, IAM, IAF. Goniometrie measurements included evaluation of flexion, range of movement, extension lag, lateral and anteroposterior stability. Dynamometric evaluation involved assessment of extension power of each leg measured with weights in the multigym. Subjective factors such as pain and other disabilities were assessed by implementing the widely accepted Knee Society clinical rating system [18]. These measurements were made both before and after treatment. The data was fed into the computer at the Center for Advanced Research and Development (CARD) and the scores were recorded as per the International Knee Society scoring system.
Informed consent as approved by the Institute’s Ethics Committee was obtained from all the patients. The knees of the subjects were exposed everyday for one hour for 21 successive days to the RFQMR beams delivered by the Cytotron, developed by CARD for the purpose. After the completion of 21 exposures, the patients were re-assessed radiologically and by other human engineering parameters. These were based on inputs for the Knee Society scoring system. The results were fed as inputs to the computer software to assess the knee society scores. Ultrasound of the knee was done to plan the dosage and map the region of interest. The assessment was repeated 30 days after completion of the treatment.
Statistical analysis
For the purpose of statistical analysis, each knee was taken as one case. Normality of the distribution of data was examined using Shapiro Wilks ‘w’ statistic. Physical attributes of male and female subjects followed normal distribution and therefore were compared using an unpaired ‘t’ Test. Treatment effect measured as Pain Score [P], Range of Movement [ROM], Total Knee Score [TKS] and Total Functional Score [TFS], exhibited significant departure from normality and therefore were compared using Wilcoxon Matched Pairs Test. Comparison of these variables between the male and female groups was done with Mann Whitney test. Spearman’s rank order correlation was attempted between physical attributes and treatment effect. All values are given as mean ±SD.
Results
The Knee Society score consisting of P, TKS, TFS and ROM were analysed. According to the Knee Society scoring, P has a maximum scale of 50 for ‘no pain’, the TKS has a maximum scale of 100 being ‘the best’, TFS also has a maximum scale of 100 and ROM has a maximum of 25 indicating ‘normal or maximum’ range of movement.
Pain
The values indicated against ‘Pain’ are inversely proportional to the degree of pain. Zero representing excruciating pain-restricting mobility. These patients were almost confined to the wheel chair and they could move their legs only while sitting in the chair. Every patient showed improvement after the course of treatment. In all the cases there was a significant abatement of pain after the third or fourth day of treatment and the pain progressively reduced during the course of exposure to RFQMR (Fig 3).
The histograms shown below depict centre points as median values, margins of boxes represent 25% and 75% percentiles and whiskers as minimum and maximum values in all graphical representations.
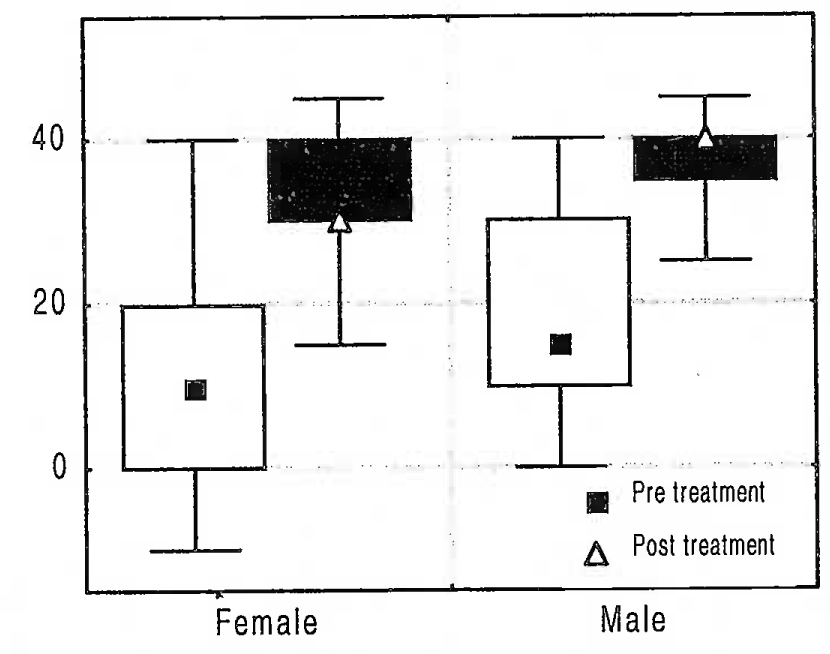
- Pain Score
Range of Movement
The range of movement increased progressively in every patient, the graph below shows the change in ROM during the course of treatment (Fig 4).
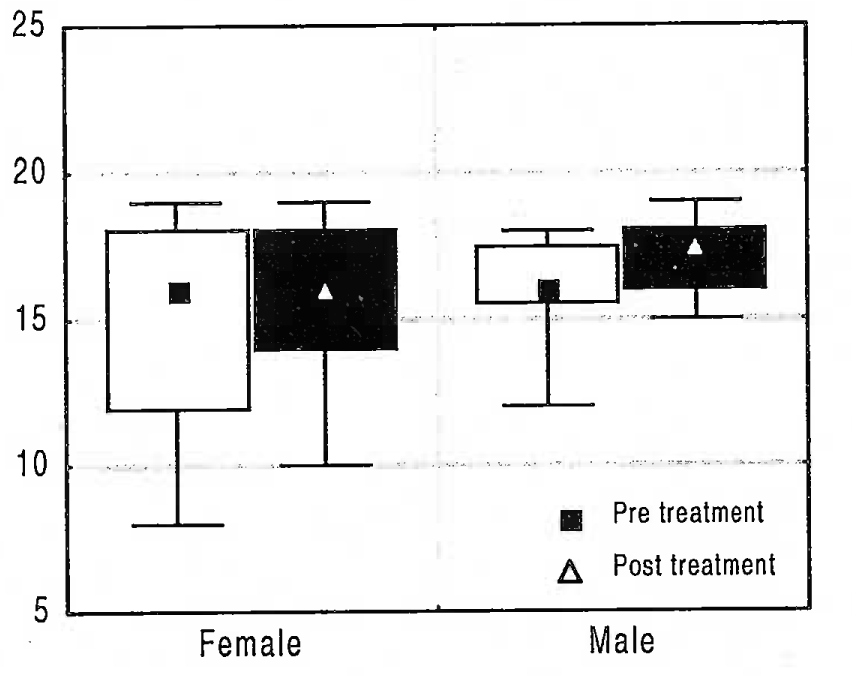
- Range of Movement
Total Knee Score and Total Functional Score
TKS and TFS improved spectacularly in all the patients, who were able to walk comfortably for considerable distances at the end of the treatement (Fig 5 and 6).
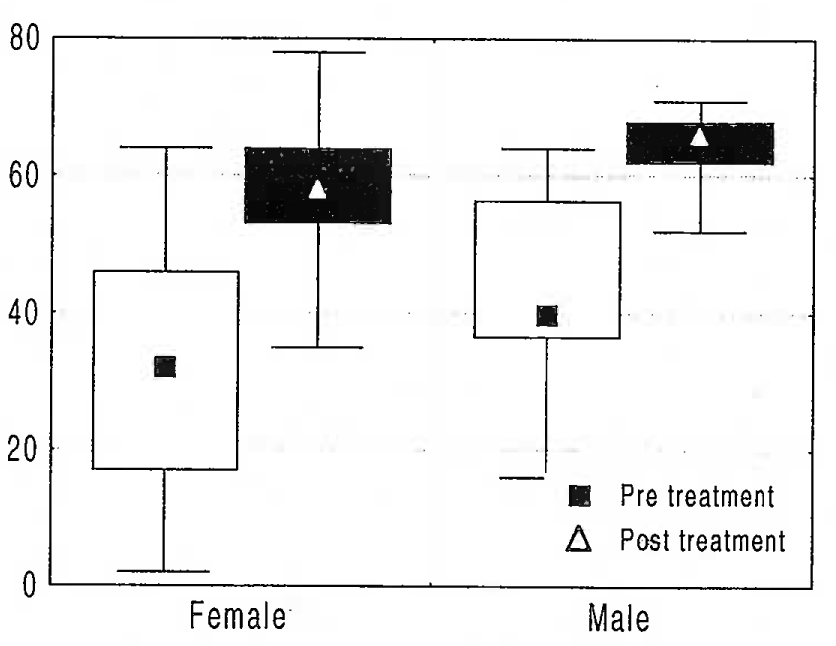
- Total Knee Score
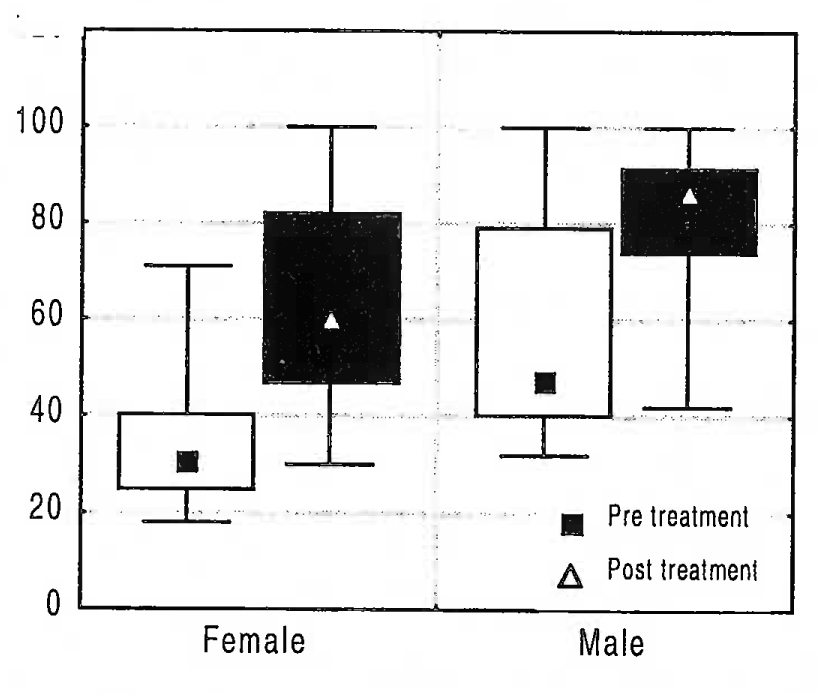
- Total Functional Score
While in younger patients the relief was evident within a couple of days of treatment, the rate of relief was slower in older patients who experienced a significant degree of relief on the 6th or 7th day of treatment. However at the end of the treatment the older patients had better TKS and P.
Further, patients with radiologic ally severe osteoarthritis improved symptomatically better than those who had mild to moderate osteoarthritis. This probably is due to the fact that a small change in these subjects would produce a great amount of symptomatic relief. Evidently, age of the patient plays an important role in the rate and degree of relief. TKS and P showed significant inprovement in older patients. Patients with mild to moderate osteoarthritis reported fairly fast improvement in their pain and walking abilities midway during the treatement.
Dynamometry
Dynamometry was done on all the patients to assess the load bearing capacity of the knee joint. After 21 days of treatment with RFQMR, most patients could push 2 to 3 times the weight they could push before the treatment, indicating that the power of the leg from the thigh to the ankle as revealed by the extension pressure of the whole leg had improved considerably. In other words, they had greater control over their knee joint.
The histogram indicating the dynamometry outcomes before and after the treatment is indicated below (Fig 7).
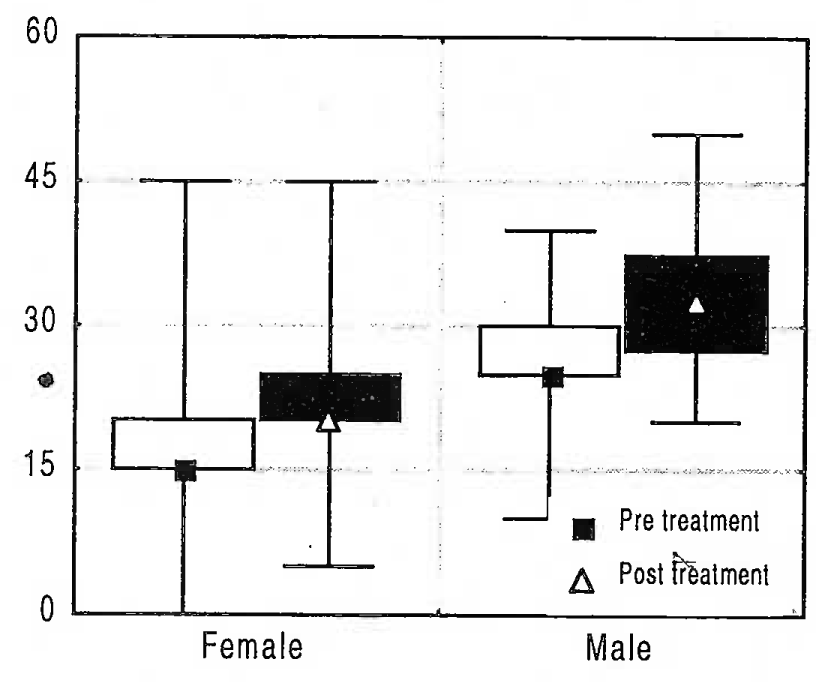
- Dynamometry
The two gender groups were comparable in age, male subjects were taller and heavier as in Table 1 (p=0.756, 0.000 and 0.011 for age, height and weight, respectively; unpaired student’s ‘t’ Test).
| Age (yrs) | Ht (cms) | Wt (kgs) | n | |
|---|---|---|---|---|
| F | 58±7 | 154±7 | 73±13 | 25 |
| M | 59±6 | 167+4 | 86±12 | 10 |
| Pooled | 59±7 | 157±9 | 77+14 | 35 |
Correlation of Patient Attributes with Treatment Benefit
Effect of treatment had no correlation with height or weight. However, age correlated significantly with improvement (difference between pre and post values) in terms d&P and TKS (Table 2).
| Pre Treatment | Post Treatment | p** | |
|---|---|---|---|
| P | 14 ±.14 | 35 ±8 | 0.000 |
| ROM | 15 ±3 | 16 ± 2 | 0.001 |
| TKS | 36± 17 | 60 + 9 | 0.000 |
| TFS | 42 ±20 | 68 ±21 | 0.000 |
P, TKS, ROM, TFS and dynamometry did not show any correlation with height, weight or age (Table 3). The statistical treatment here was using Spearman’s Rank Order Correlation, considered appropriate for the data type. All the other correlations were non-significant.
Gender Difference in the Responsiveness to Treatment
There was no gender difference in response to treatment as evident from results of Mann Whitney U Test (p=0.346, 0.158, 0.269 & 0.351 for P, ROM, TKS and TFS, respectively). Details of these data are hence not presented.
Discussion
Hyaline cartilage, which forms a cap on the long bones and the inner surface of the patella in the knee joint, is constantly produced from the chondroblastic layer. This process is continuously activated by the constant use of the joint. Disuse atrophy, which is a well known biological phenomenon, applies specially to the knee joint since it is the most important load bearing joint in the human body. The disuse of the joint shows its effect in the form of degeneration of cartilage in the articular surfaces of the bones in the knee joint. Overuse, constant impact and injuries lead to early onset of degenerative change. The rate and extent of degeneration depend on the degree of disuse and the process of aging in the individual. Consequently, older persons exhibit a rapid progress of osteoarthritis because the regenerative capacity of the chondroblasts is progressively reduced with age and sedentary habits. Joint pain sets in, this in turn reduces mobility causing disuse atrophy of the supporting muscles leading to increased loading and the cartilage degenerates further and thus a negative cycle sets in. Hence, the earlier the disease is diagnosed and treated, the greater is the effectiveness in the activation and regeneration of the cartilage.
RFQMR stimulates the chondrocytes and initiates the regeneration process, reduces pain and increase ability of the joint, thus reversing the regauve cycle. This study demonstrates that use of RFQMR treatment for osteoarthritis decreases pain, increases mobility, stability and power of the knee joint and helps normalise the life of an osteoarthritic patient. The patients were followed up after 30 days of the treatment and showed no deterioration in their Knee Scores or pain status.
Conclusion
Younger subjects had earlier subjective and objective relief, which was almost complete at 21 days.
Subjects with lower pain scores (i.e. more pain) showed greater subjective improvements.
No gender difference to treatment was seen.
No significant difference in status at the end of treatment and at one month was noted.
Exposure of the knee cartilage to RFQMR is an effective method of treatment and can be a new line of treatment for osteoarthritis.
References
- Biological and clinical effects of low frequency electric and magnetic fields, Australias. Phys and Engl Sci Med. 1980;3:182-192.
- [Google Scholar]
- The effect of combined AC/DC magnetic fields on resting articular cartilage metabolism.
- Direct medical costs unique to patients with arthritis. Journal of Rheumatology. 1997;24:719.
- [Google Scholar]
- Physical Basis of coherent radiations from bio molecules In: Proc. P’ Inti. Symp. on photon Emission from Biological Systems. 1987. p. :63-95. in:
- [Google Scholar]
- Symposium explores mechanisms for ELE electromagnetic Bio effects. Frontier Perspectives. 1991;2(2):1-24.
- [Google Scholar]
- Transcriptions and translations in cells exposed to extremely low frequency electromagnetic fields. Bioelectrochem. Bioenerget. 1991;25:335-355.
- [Google Scholar]
- Effect of weak pulsing electromagnetic fields on neural regeneration in the rat. Clinical Orthop and Related Research. 1983;181:283-290.
- [Google Scholar]
- Membrane electroporation: Toward a molecular mechanism.
- Bests. Electromagnetic Man. London: JM Dent & Sons; 1989.
- Chapman D, Wallach DN, eds. in Biological membranes, Vol. II. London: Acad Press; 1973. p. :253.
- Textbook of Medical Physiology. Philadelphia: WB Saunders Comp; 1976.
- Electroinsertion of proteins into membranes: A novel approach to the study of membrane receptors, Harvard Univ. USA. Electricity and magnetism in biology and medicine. USA: San Francisco Press, Inc.; 1992.
- A continuum model of cartilage electrokinetics and correlation with experiments. J Biomech. 1987;20:629-39.
- [Google Scholar]
- Pulsed Signal Therapy (PST) stimulates mitosis of human chondrocytes in culture.
- A Double blind trial of the clinical effects of pulsed electromagnetic fields in osteoarthritis. J Rheumatol. 1993;20:456-60.
- [Google Scholar]




