
Translate this page into:
Retrospective analysis of medical information records for 6 years of a national carrier in a Middle East country

*Corresponding author: Umesh Kumar Kadubasavaiah Bhagavath, Department of Civil Aviation, Rusayl Health Centre, Muscat, Oman. umeshyash7@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bhagavath UK. Retrospective analysis of medical information records for 6 years of a national carrier in a Middle East country. Indian J Aerosp Med 2023;67:28-34. doi: 10.25259/IJASM_9_2021
Abstract
Objectives:
Flying as a passenger without any disease or disability in a commercial airline poses no threat to the carrier or the passenger. People with diseases travel from one part of the country to another part or a different country for better treatment is called medical tourism. Patients with diseases are exposed to various stresses of aviation such as hypoxia, noise, vibration, and effects due to the expansion of gasses. Every airline has medical information form (MEDIF) form for all ill or incapacitated passengers.
Material and Methods:
Systematic analysis of medical information of a National carrier of a Middle East country was done for the past 6 years. A total of 44346 MEDIF forms were cleared from January 1, 2013, to December 31, 2018. One for every 665 passengers and 0.13 per flight. More than half of the request was from male passengers.
Results:
Most MEDIF passengers requested wheelchair holding till the cabin. It was 62.46%. The musculoskeletal system was the most frequently affected in the requested MEDIF Form. It constituted nearly 41% of all the MEDIF cases. Stretcher cases constituted 8.2% of all MEDIF cases.
Conclusion:
Results from the study threw light on the systems frequently affected by MEDIF clearance and the necessary precautions to be taken before clearing the MEDIF cases.
Keywords
Medical information forms
Incapacitated passenger
Wheelchair
Musculoskeletal system

INTRODUCTION
Worldwide 4.1 billion passengers flew by commercial airlines in the year 2017.[1] Flying as a passenger without any disease or disability in a commercial airline poses no threat to the carrier and passenger. People travel from one to another country for better healthcare and management of diseases. This could be due to the non-availability or scarcity of specialized investigative procedures including the economic viability of the treatment process in the parent country; is called medical tourism. Domestic medical tourism encompasses people who travel from one to another city for better medical care within their homeland.[2] There is an almost three-fold increase in passengers traveling with diseases because of an increase in longevity and improvement in the economic status worldwide compared to the last decade.[3] Patients with diseases and disabilities are exposed to the stresses of aviation such as reduced cabin pressure, noise, vibration, and effects due to the expansion of ambient gas. Some of the diseases aggravated during the flight caused increased morbidity and mortality in certain cases.[4] Sick passengers pose a threat not only to co-passengers but also to airline crews specially pilots and in-flight attendants in case of the onboard sudden death of a patient-passenger. This will add on to the operating cost of the aircraft and delay for fellow passengers because of diversions.[5] To streamline the diseased passenger travel by air, every airline uses Medical information form (MEDIF) as laid down by International Air Transport Association (IATA).
IATA resolution 700 specifies selectively passengers with disabilities or diseases needing preflight medical clearance to board commercial flights. IATA has created a special incapacitated passenger handling advice form.[6] This is divided into two parts; Part-1 to be completed by the airline’s medical department and Part-2 also known as MEDIF, to be filled by the attending physician with all relevant medical data, date, and nature of diagnosis including special health needs or requirements on-board. In this national airline, a single MEDIF form is to be filled out for each passenger and there is no frequent medical card (FREMEC) in use. FREMEC card is carried by disabled persons who require little or no special assistance during air travel. All types of patients are treated as MEDIF cases and all are generally cleared by the Aviation Specialist of National Carrier. Considering the upward trend of air travel by indisposed passengers, it was decided to make an effort to check the MEDIF record for the past 6 years, that is, January 2013–December 2018 of a national carrier in a Middle East country.
MATERIAL AND METHODS
In this retrospective database study, a systematic review of all the MEDIF cases of National Carrier was done for 6 years from January 01, 2013 to December 31, 2018. MEDIF forms for the sick passengers were filled by the treating physician at their clinics or Hospitals. Detailed clinical condition of the passenger was assessed based on the MEDIF record and the clearance was given as per the request by the passenger. Filled MEDIF forms were submitted at the National Carrier Office at respective stations. These MEDIF forms are then scanned and sent to the call center. From the call center, these forms were sent to the National Carrier Clinic for clearance. These forms are cleared by the Aviation Medical Specialist at the National Carrier Clinic. Approved forms are then sent back to the call center which in turn sends the requirement to various departments for oxygen cylinders, stretchers, wheelchairs, and special equipment, respectively. The collected data were analyzed on a customized excel sheet.
The work considered the following parameters for study to incorporate details of the patient’s medical, health, and other needs.
Destination: There are two types of destinations for passengers; domestic; and international. The domestic destination has been used by passengers mainly coming from other cities within the country travelling for definitive treatment at capital region hospitals. International destination is sought by incoming/ outgoing passengers seeking medical treatment in a different country.
-
Total number of clearances as per the age
<2 years
2–10 years
10–18 years
18–60 years
Above 60 years.
-
Sex distribution of the same is as follows
Male
Female.
-
Sector of travel was divided in short and long haul flights
Short haul-flight time <3 h
Long haul-flight time of more than 3 h (long haul).
-
Passengers who can sit upright are classified into three categories, namely, Wheelchair holding with rest (WCHR), wheelchair till steps (WCHS) and wheelchair holding to cabin (WCHC).[7] Further detail as follows.
WCHR: Passenger can ascend/descend steps and make their own way from cabin seat but requires wheelchair for coming from distance to aircraft, that is, across ramp, gate, or to lounge as appropriate
WCHS: Passenger cannot ascend/descend steps, but can make their own way to and from cabin seat; requires wheelchair for distant reach to and from aircraft/lounge and must be assisted in climbing up and down steps
WCHC: Passenger totally immobile; requires wheelchair from/to aircraft/mobile lounge and must be carried up and down steps.
Lying/Stretcher cases were analyzed independently with or without oxygen.
Diseases were analyzed depending on the system involved such as cardiovascular system (CVS), central nervous system (CNS), musculoskeletal, and other systems.
Analysis
Destination
MEDIF clearances revealed that 72% of the destination was India compared to only 10% to domestic location [Figure 1]. Next destination was Thailand 8%. Other destinations such as Munich, London, Lahore, Karachi, and Manila accounted for 10%. This could be because of the tie-up of the hospitals in the originating country with hospitals in India including superior and economical medical treatment compared to other destinations.

- Destination patient passengers.
Destination of patient-passengers
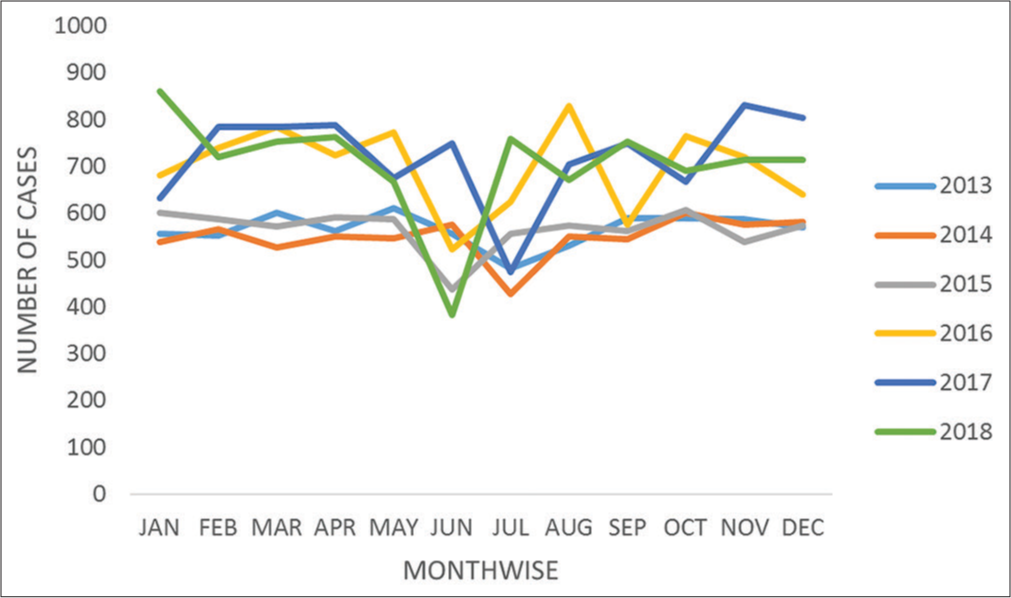
A total of 44,346 MEDIF cases were cleared by the national carrier in a span of 6 years from January 2013 to December 2018 [Table 1 and Figure 2]. Total MEDIF cases year and month wise is shown in [Table 2]. On the total MEDIF clearances, it was found that on average 755 used to be cleared in a month and there was a dip in the medical clearances during the month of Ramadan.
- Distribution of medical information form cases.
| Details of passengers, flights and patients | Year | Total | |||||
|---|---|---|---|---|---|---|---|
| 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | ||
| No. of passengers in 100 | 40995 | 5052 | 6366 | 8283 | 8606 | 9030 | 78332 |
| No. of flights | 40481 | 47823 | 50616 | 51952 | 54746 | 57646 | 303264 |
| No. of MEDIF cases | 6672 | 6583 | 6602 | 7380 | 8649 | 8460 | 44346 |
| Cases per flight | 0.16 | 0.13 | 0.13 | 0.14 | 0.15 | 0.14 | 0.15 |
| Patients per million passengers | 1627 | 1303 | 1037 | 987 | 1004 | 936 | 1462 |
MEDIF: Medical information form
| Year | January | February | March | April | May | June | July | August | September | October | November | December | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2013 | 556 | 553 | 602 | 563 | 612 | 557 | 482 | 531 | 589 | 590 | 587 | 570 | 6792 |
| 2014 | 539 | 567 | 527 | 551 | 547 | 577 | 428 | 550 | 546 | 601 | 576 | 583 | 6592 |
| 2015 | 601 | 588 | 573 | 591 | 588 | 437 | 556 | 574 | 562 | 607 | 539 | 574 | 6790 |
| 2016 | 682 | 740 | 785 | 725 | 773 | 524 | 625 | 829 | 576 | 765 | 720 | 640 | 8384 |
| 2017 | 633 | 785 | 785 | 788 | 675 | 750 | 474 | 705 | 750 | 668 | 832 | 804 | 8649 |
| 2018 | 860 | 720 | 754 | 764 | 667 | 384 | 760 | 672 | 754 | 692 | 714 | 715 | 8456 |
MEDIF: Medical information form
Total number of MEDIF clearances as per the age are reflected in [Figure 3]. Proportion of MEDIF cases were 4.88% among <2 years, 5.99% in 2–10 years, 3.94% in 10–18 years, 15.8% in 18–40 years, 42.3% in 40–60 years, and more than 27.19% among 60 years and above. Least number of passengers was noted in 10–18 years group as against most in the age bracket of 40–60 years.
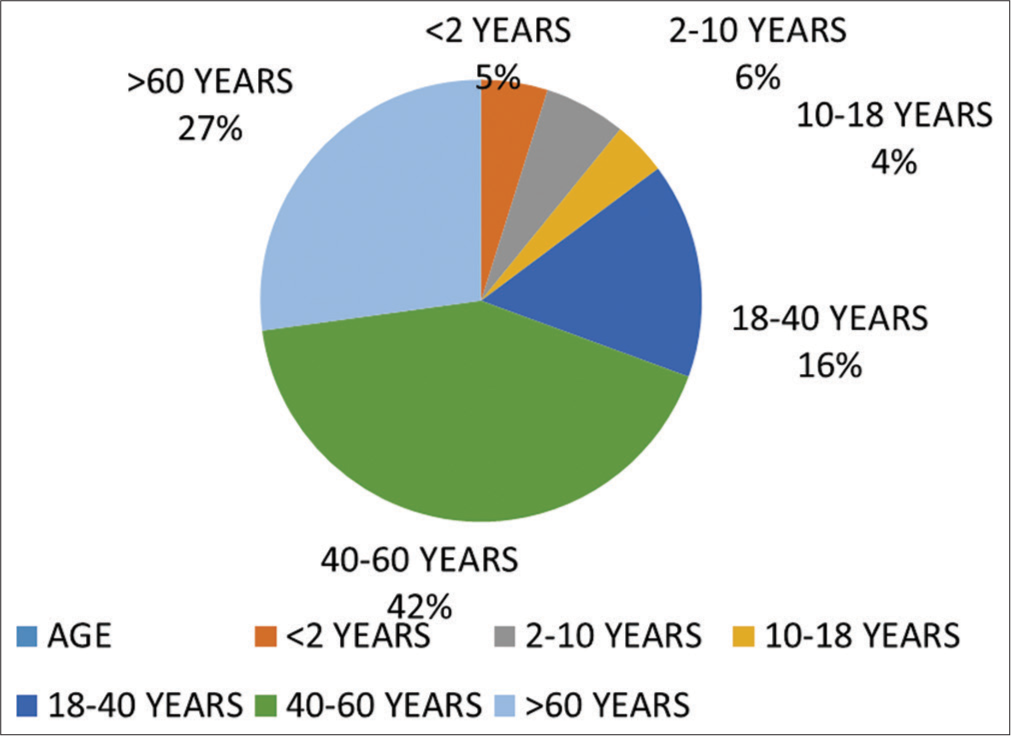
- Age wise distribution of medical information form cases.
Male constituted 56% of total evacuation compared to 44% females. Short haul flights constituted only 18% of total against 82% being long haul flights.
Distribution of cases according to allotment of various requests is given as [Table 3 and Figure 4].
| WCHR (%) | WCHS (%) | WCHC (%) | STRETCHER (%) | BASINET (%) |
|---|---|---|---|---|
| 6.42 | 22.18 | 62.46 | 8.21 | 0.99 |
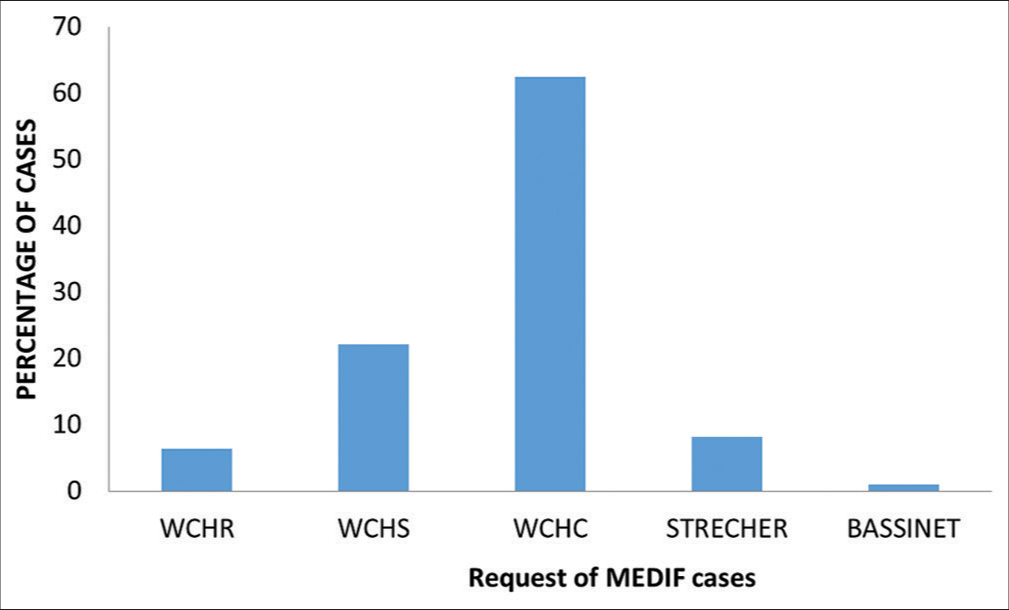
- Distribution of cases.
Stretcher was needed by nearly 8.21% of the total MEDIF cases. Oxygen was requested by 32% of sick passengers. Patients with diseases such as total hip replacement, treated and stabilized stroke, vertebral fracture, pelvic fracture, head injury, hypertension/NIDDM with end stage renal disease (ESRD), chronic liver disease, and paraplegia did not ask for any oxygen requirement. Oxygen was requested in post-cardiac arrest, congenital heart disease, and tracheostomy with multiple organ failure, pneumothorax, and lung transplant.
Distribution of MEDIF cases according to various systems are reflected in [Table 4 and Figure 5].
| Disease system affected | Percentage |
|---|---|
| CVS | 31.36 |
| CNS | 18.02 |
| RS | 2.08 |
| GIT/Endocrines | 2.07 |
| Musculoskeletal | 41.17 |
| Urogenital | 3.12 |
| Haemopoietic | 1.08 |
| Eye | 0.3 |
| MISC | 0.7 |
MEDIF: Medical information form, CVS: Cardiovascular system, CNS: Central nervous system, RS: Respiratory system, GIT: Gastrointestinal tract, MISC: Miscellaneous
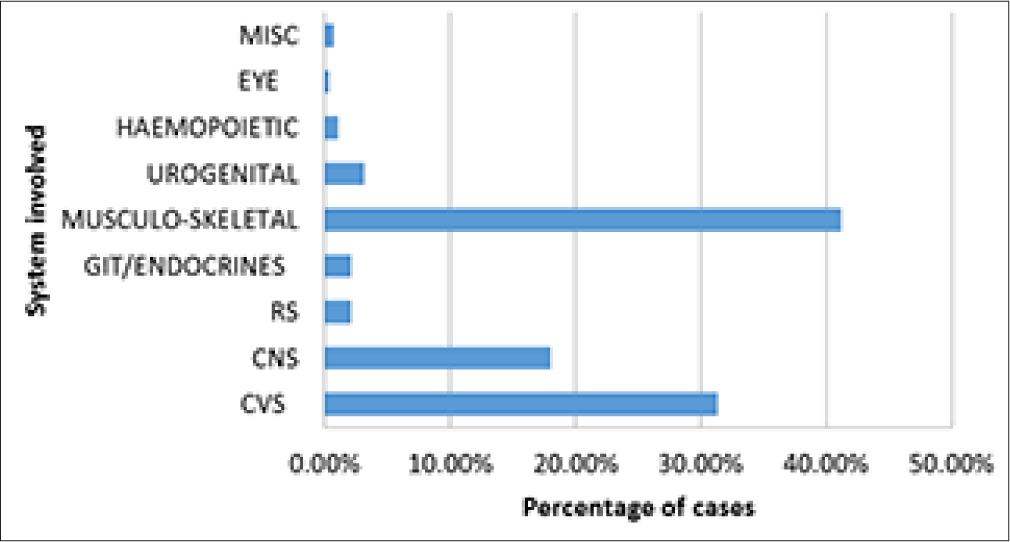
- Distribution of cases system-wise.
Oxygen calculations
Oxygen was requested by 9% of the total passengers. Oxygen requirement varied from 2 L to 8 L/min. Aircraft oxygen cylinder usually has a capacity of 625 L. The last 75 L are generally not available for the patients. Calculation of oxygen requirement entails one cylinder at the rate of 2 L/min lasts for 4.5 h and at the rate of 4, 6, and 8 L/min will last for 2.5, 1.5, and 1.16 h, respectively. The above calculations are applied for the cases requiring oxygen. In general, one additional oxygen cylinder is provisioned along with the required oxygen to cater for the contingencies such as diversion and delay of flight.
Diseases of various systems by MEDIF clearances
Musculoskeletal system: This accounted for nearly 41% of the total MEDIF cases. Osteoarthritis of the knee, knee surgery, and total knee replacement constituted 36% of all the musculoskeletal disorders. Next commonest (23%) was Lumbago and post-surgical cases for backache such as discectomy and laminectomy. Fracture of the lower limb of different types was nearly 18%. Fracture of upper limb constituted 8%. Total hip replacement was seen in 8% of cases. Cervical spondylitis and cervical vertebral fractures included 4%. Other musculoskeletal disorders such as pseudo hypertrophy and muscular dystrophies recounted for 3% of total musculoskeletal cases.
CVS: This comprised of 31.36% of all MEDIF cases. Myocardial infarction (MI), pre-Percutaneous transluminal coronary angioplasty (PTCA) and post-PTCA, angiogram, and coronary artery bypass graft (CABG) accounted for nearly 50% of the cardiovascular cases. Simple hypertension and complication of hypertension constituted nearly 18% of the cardiovascular cases. Valvular diseases and valve Replacement surgeries counted for nearly 8%. Heart blocks and pacemaker implantation constituted 8% of CVS cases.
CNS accounted for 18.02% of all MEDIF cases. Seizures and its surgical/medical management accounted for nearly 38% of all CNS patients who travelled in this category. Stroke and hemi-paresis accounted for 26%. Brain tumors with pre/ post-surgical management constituted 16% of all CNS cases. Intracranial surgeries and traumatic brain injuries surgeries accounted for 15% of all CNS cases.
Urogenital system (UGS) represented 3.12% of all MEDIF passengers in which renal and ureteric stones topped the list (68%). ESRD with associated risk factors noted for nearly 24% of UGS cases. Renal transplant and miscellaneous surgeries accounted for 8% of UGS patients.
About 2.08% of the MEDIF cases were affected by the diseases of respiratory system (RS) of which chronic obstructive pulmonary disease (COPD) and bronchial asthma accounted for nearly 62% besides bronchiectasis in 22% of the cases. Pneumothorax and pneumonia were present in 14% of cases. There were two lung transplant MEDIF cases.
Gastrointestinal system and endocrinal system constituted 2% of all MEDIF cases. GI cases included mainly hiatus hernia, Crohn’s disease, intestinal polyposis, and chronic gastritis. Endocrinal diseases were non-insulin dependent diabetes Mellitus/insulin dependent diabetes mellitus (NIDDM/IDDM) which accounted nearly 75% with Hypo/Hyper-thyroidism making up the remaining 25% of endocrinal cases.
Sickle cell disease, bone marrow pre-transplant, and thalassemia were frequent diagnosis in the hematopoietic system presenting 1% of total MEDIF cases.
Eye diseases accounted for nearly 0.3% of the total MEDIF cases. Corneal ulcer, irido-cyclitis, and retinoblastoma were the common diagnosis.
Malignancies such as leukemia, carcinoma of thyroid, CA breast, CA colon, and CA prostate counted for 0.7% of the total MEDIF cases. Carcinoma of colon was the most frequent amongst malignancies. Miscellaneous group had patients for regular/periodic medical checks and corrective surgery for obesity.
DISCUSSION
Fitness for the air travel is a task by itself as many passengers are not aware of the consequences of the air travel on the passengers. Passengers with diseases pose a threat not only to other passengers but also to the pilot and the airline in case of on board death. This will add on to the operating cost of the aircraft and delay to the fellow passengers because of diversions.
National carrier carried nearly 8.6 million passengers in the year 2017. Total number of flights varied from 40,481 in 2013 to 54,746 in 2017[8]. Total MEDIF cases per flight varied from 0.13 to 0.16. National Carrier MEDIF cases have been comparatively large compared to Oman Airlines study by Jorge et al.[9] Total number of MEDIF cases are one in every 637 passengers compared to the 1/10,935 passengers in the former study. This is because of two reasons. First, most of the latest and advanced treatment options for the citizens are available at Capital city; hence being referred from the periphery to the capital city. Second, large contingencies of emigrants do work in this Middle East country in construction and infrastructure industry and are sent back to their country of origin following any injuries/ accidents by referral to linked hospitals for advanced care and treatment.
Commercial flights usually cruise at an altitude of 7010–12498 meters above the mean sea level (msl) with passenger cabin pressurized to an altitude of 1424–2438 m. Cabin pressurization to an altitude of 2438 m above MSL reduces the atmospheric pressure of the cabin resulting in the concomitant decrease in arterial oxygen partial pressure (PaO2) from 95 to 60 mm of Hg. In healthy passengers, these parameters could lead to 3–4% decrease in oxygen saturation. However, many passengers with pre-existing cardiac, pulmonary, and hematological conditions having reduced PaO2 experience further reduction of oxygen saturation due to low cabin pressure, which deteriorates further with extended flight times. About 18% of passengers with COPD experience mild respiratory distress during flight.[10]
Oxygen supplementation is recommended for passengers either having the resting oxygen saturation of 92% and lower or if the expected PaO2 on-board is <52–55 mm of Hg. The aerospace medical association (AMA) guidelines suggest that sea level blood gas estimation or pulmonary function testing as the gold standard; AMA recommends in-flight oxygen for individuals with a sea level PaO2 of 70 mm of Hg and lower or with an expected in-flight PaO2 of 55 mm of Hg or lower. Some evidence suggests that these guidelines need revision as predictive equation often inaccurately estimate in-flight PaO2.[11,12] Our experience in clearing the MEDIF cases suggests that maintenance oxygen is required in cases such as bronchial asthma and post-MI where 2–4 L of O2/min has generally been requested. In case of pulmonary fibrosis or bronchiectasis, 6 L/min would be required. In most cases where the passenger was on ventilator, 8 L/min was requested. Airlines as a policy, provides only oxygen on-board and all the portable battery operated medical equipment need to be carried by medical attendant for its use in-flight. All stretcher cases requiring oxygen need to be escorted by a medical attendant such as a nurse or a doctor.
Gas in the body cavities is also affected by the cabin pressure. According to the Boyles law, at a constant temperature, volume of the gas is inversely proportional to the pressure. Therefore, with reduction in cabin pressure, expansion of gas takes place in the semi-closed and closed cavities like middle ear and paranasal sinuses (PNS). Middle ear contains around 8–10 mL, PNS contain about 30–50 mL (Maxillary – 15 mL, Frontal – 8 mL, Ethmoidal – 3 mL, and Sphenoid sinus – 5–8 mL) and gastrointestinal tract contains about 400 mL of air. Expansion of gas in closed body spaces in a normal passenger may not make any difference but in an operated patient where the gas expands by 30% of volume, can result in wound dehiscence and even bowel perforation. Hence, 10 days of post-operative recuperation (POR) is needed in all cases of intra-abdominal surgery and 24–48 h following a laparoscopic surgery.
Nearly 133 MEDIF cases were rejected over a period of 6 years constituting 0.003% of all MEDIF cases. Mostly the MEDIF forms were not filled properly and many were asked to resubmit later following surgeries with POR <10 days, MI with <7 days of stabilization, unresolved pneumothorax, and hemorrhagic cerebrovascular accidents having <10 days stabilization. Rejection rate in the present work is quite low compared to findings of earlier study[9] that annotated a rejection of 3.1%.
There was deterioration in 18 MEDIF cases which caused in-flight medical emergencies and were managed by oxygen and other medication. This accounts for one per every 16,848 flights which is much higher than the figures documented by Goodwin.[13] Three cases warranted diversion and off-loading of the patient. There were two deaths among MEDIF cases in the above mentioned period where in one patient of ischemic heart disease with cardiac failure could not be revived even with on-board cardiopulmonary resuscitation (CPR). Another 76-year-old passenger in wheel chair (WCHC) died on-board but cause of death could not be ascertained.
The main objective of MEDIF clearance is to ensure that the diseased passenger reaches his destination without any untoward incidences. It is also important that disease does not get aggravated during flight causing undue stress to the pilot and cabin crew. It is important for the doctor, who fills the MEDIF form, should clearly mention the diagnosis and any specific requirement that may be needed during flight. Care to be exercised while clearing the patients with physical disabilities having plaster cast immobilization which should not interfere with egress of passengers during the emergency evacuation. Recent MI within 7 days was not cleared due to expected life-threatening complications that usually occur within 7 days.[14] Almost all the psychiatric cases were cleared with escort and were advised to take the sedatives before flight. All the MEDIF passengers with Uro-bag were advised to empty the bag before flight. All respiratory cases having <200 L/min PEFR were rejected due to compensation of lung during flight.
CONCLUSION
MEDIF clearances require considerable amount of knowledge of aviation medicine for safe transportation of patients from one sector to another. Fractures and diseases of limbs constitute the major share of patients travelling with MEDIF. Diseases of the CVS and RS require special attention before clearing for flying as passenger with MEDIF. The present work attempted a record analysis for data accumulated over 06 years for a particular airlines. The future research in similar directions is recommended to substantiate the finding of the present study.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Travelers Numbers Reach New Heights. 2018. Available from: https://www.iata.org/pressroom/pr/pages/2018-09-06-01 [Last accessed on 2021 Mar 13]
- [Google Scholar]
- Available from: https://www.medicaltourismassociation.com/en/medical-tourism [Last accessed on 2021 Mar 13]
- Fitness to Fly-medical Clearance Required. In: Cabin Health 2002 Cabin Health Conference. Geneva: International Air Transport Association; 2002.
- [Google Scholar]
- Resolution 700: Acceptance and Carriage of Invalid Passengers. Canada: International Air Transport Association 2020 Available from: https://www.eagosh.org/eagoshfiles/articles_presentations_infos/sars/iata_who/iata_reso_700_e.pdf [Last accessed on 2021 Mar 13]
- [Google Scholar]
- Travel Medicine In: Proceedings of the First Conference of International Travel. 2018. p. :564.
- [Google Scholar]
- Resolution 700 Acceptance and Carriage of Incapacitated Passengers Canada: International Air Transport Association; 2020.
- [Google Scholar]
- All Passengers this Way Airlines International. 2017. Available from: https://www.airlines.iata.org [Last accessed on 2017 Oct 12]
- [Google Scholar]
- Oman-air Annual Reports 2013-2017. 2017 Available from: https://www.omanairreports.com [Last accessed on 2020 Nov 17]
- [Google Scholar]
- Preflight medical clearance of ill and Incapacitated passengers: 3-year retrospective study of experience with a European airline. J Travel Med. 2005;12:306-11.
- [CrossRef] [Google Scholar]
- Hypoxemia during air travel in patients with chronic obstructive pulmonary disease. Ann Intern Med. 1989;111:362-7.
- [CrossRef] [Google Scholar]
- Flight assessment in patients with respiratory disease: Hypoxic challenge testing vs. predictive equations. QJM. 2007;100:361-7.
- [CrossRef] [Google Scholar]
- Hypoxaemia in chronic obstructive pulmonary disease patients during a commercial flight. Eur Respir J. 2005;25:725-30.
- [CrossRef] [Google Scholar]
- Safety of commercial air travel following myocardial infarction. Aviat Space Environ Med. 1996;67:976-82.
- [Google Scholar]




