Translate this page into:
Protection by AGSM: Our Experience
Abstract
Anti-G Straining Maneuver (AGSM) is a means of improving the aircrew G tolerance. A well done AGSM is said to provide a 4G protection besides the 1G from AGS. Institute of Aerospace Medicine, Indian Air Force (IAM, IAF) has been conducting High G training of the aircrew since 1991. The training objective is to teach the aircrew a correct AGSM (L-l Maneuver) in a safe and a controlled environment. The amount of protection afforded by this AGSM on the G tolerance of the aircrew was explored in this study.
Method:
Subjects were given 02 centrifuge exposures [Gradual Onset Run (GOR) 0.1G/s] on two different days. The end point was subjective Peripheral Light Loss (PLL) of 52-56°. On Day 1 after determining the relaxed G tolerance they were asked to do normal straining (as they do in the aircraft) until PLL. On day 2 they were to do AGSM as taught in IAM, IAF on experiencing the PLL. ECG and heart rate was recorded. One way analysis of variance (ANOVA) was performed using Tukey’s Multiple Comparison Test. A level of p< 0.05 was considered as significant.
Results:
The relaxed and straining G tolerance of the subjects on Day 1 was 4.4±0.6G and 6.5±1.1G respectively and on Day 2 relaxed G tolerance was 4.3±0.7G and G tolerance with AGSM was 7.3±0.7G The protection offered by straining was 2.l±0.7G and that offered by trained AGSM was 3.0±0.1G. Statistical analysis shows significant difference in the protection offered by trained AGSM in comparison to the straining.
Conclusion:
The present study was done to examine the protection given by AGSM training to aircrew undergoing OPTRAM-F course at IAM. A w ell done AGSM is said to provide up to 4G protection and the present study shows that the AGSM training at IAM provides an average of 3G protection.
Keywords
Straining G level tolerance
AGSM

Introduction
Flying high performance aircraft exposes the aircrew to high sustained accelerations mainly in the +Gz axis. The ability to withstand the high Gz exposure is mainly governed by the arterial pressure [1,2]. The arterial pressure at the heart level must be increased to overcome the G induced hydrostatic pressure gradient. The mean arterial pressure at the heart level needs to be elevated to around 230-280 mmHg from the baseline of 100 mm Hg to tolerate the exposure of +9Gz. The aircrew has an innate G tolerance of around 4G. A well fitted Anti-G Suit (AGS) provides 1G protection. A well done Anti-G Straining Maneuver (AGSM) performed by the aircrew is said to provide 4 G protection. The AGSM comprises of muscular contractions of the abdomen and legs, and specialized respiratory techniques. The large-muscle component consists of strong, sustained isometric contractions of the muscles of the abdomen and limbs, producing a reflex increase in blood pressure and a mechanical decrease in peripheral pooling. The respiratory component involves use of Valsalva and related respiratory manoeuvres to raise intra-thoracic pressure and hence the arterial pressure at the heart. These manoeuvres are taught to pilots, who learn to tense all major muscle groups while adopting a breathing pattern that involves straining against a closed glottis for 3 to 4 seconds, taking a quick breath and returning to straining [3]. Regular practice is required to maximize both skill and stamina for these manoeuvres, and strength training of major muscle groups has been found to significantly increase tolerance for sustained high-G profiles. IAM. IAF has been conducting High G training of the aircrew since 1991. The training objective is to teach the aircrew a correct AGSM (L-1 Maneuver) in a safe and a controlled environment. The present study was performed to study the amount of protection afforded by this AGSM.
Aim
The aim was to study the amount of G protection given to the aircrew by the AGSM (LI maneuver) trained at IAM, IAF Bangalore.
Material and Methodology
Subjects
A total of 20 healthy, young, male aircrew participated in the study. One aircrew could not complete the profile and hence was excluded from the study. Their physical attributes were as follows: height 174.1 ± 5.3 cms (Range 165-184 cms). weight 71.7± 6.5 kgs (Range 59-80 kgs); the values are Mean ± SD. The subjects were informed about the experimental protocols and an informed consent was taken. (Table 1 refers).
| Parameter | Mean | SD | Range |
|---|---|---|---|
| Age (yrs) | 26.7 | 5.2 | 21-35 |
| Height (cm) | 174.1 | 5.3 | 165-184 |
| Weight (kg) | 71.7 | 6.5 | 59-80 |
| Flying experience (hrs) | 582.8 | 389.1 | 200-1300 |
Experimental Arrangements and Protocol
The study was conducted in the 8 meters radius High Performance Human Centrifuge (HPHC) at the Institute of Aerospace Medicine, Bangalore. During the runs the subjects were seated with the back reclining 15 degrees. The subjects were given 02 centrifuge exposures (GOR 0.1 G/s) on two different days. A light bar comprising of a central red light and peripheral lights at 52-56° was used for assessment of Peripheral Light Loss (PLL). The end point was subjective PLL of 52- 56°. On day 1 the subjects were given a GOR exposure at 0.1 G/s and while staying relaxed on achieving PLL they were asked to strain the way they are used to do in their aircraft. They were to leave the dead-man switch on achieving PLL while straining. On day 2, a similar GOR run (Onset 0.1 G/s) was given and on achieving PLL while staying relaxed they were instructed to do AGSM (L1 Maneuver) with counts given by the medical controller. The subjects were instructed to release the dead-man switch on achieving PLL while doing AGSM. The subjects were in their flying overalls and were not wearing any Anti-G Suit. ECG (lead I.II.III) and Heart rate was recorded during all the runs.
Statistical Analysis
One way analysis of variance (ANOVA) was performed using Tukey’s Multiple Comparison Test for comparison of G protection afforded by straining vs G protection afforded by AGSM. A level of p< 0.05 was considered as significant.
Results
The relaxed G tolerance of the subjects was 4.4±0.6G and the straining G tolerance of the subjects was 6.5± 1.1G on Day 1. The relaxed G tolerance of the subjects was 4.3±0.7G and G tolerance with AGSM was 7.3±0.7G on Day 2 (Figure 1 refers).
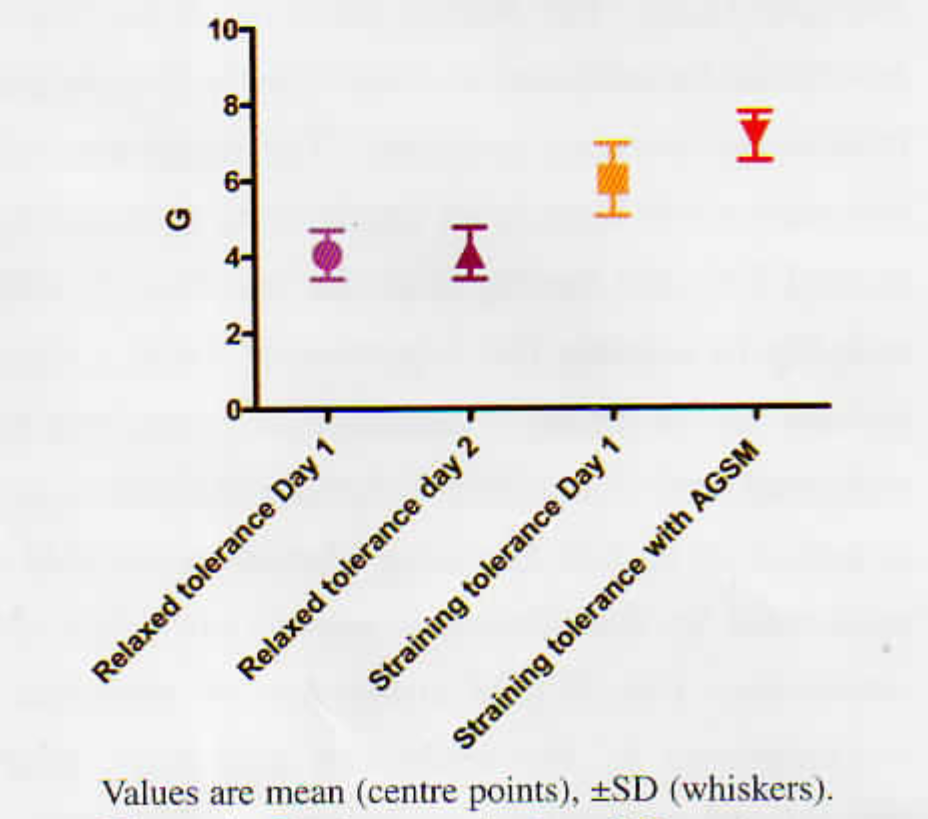
- G tolerance during different runs
Statistical analysis shows no significant difference in the relaxed G tolerances on Day I and Day 2. However, significant difference (p< 0.05) was seen between the straining G tolerance and straining G tolerance with AGSM (Table 2 refers).
| Runs | Statistical Analysis | ||||
|---|---|---|---|---|---|
| Relaxed Tolerance Day 1 (a) | Relaxed Tolerance Day 2(b) | With s training (c) | With AGSM (d) | ||
| G tolerance | 4.4±0.6G | 4.3±0.7G | 6.5±I.IG | 7.3±0.7G | a vs b Not significant c vs d Significant |
Discussion
AGSM is a learned maneuver, it must be taught to the pilots. Its importance in increasing G tolerance at 9G producing 80% of the increase in tolerance over the basic G tolerance of 4G in the high G arena requires that the pilots perform this maneuver in an extremely effective manner [3]. The simulated, safe and controlled environment of a human centrifuge helps to train the aircrew to perform a correct AGSM.
It was in 1924 in France that the use of muscular tensing and increasing the intra-thoracic pressure by pilots to improve G tolerance was originated. The in-flight application of a muscle straining maneuver is attributed to Stainforth of England in 1933 [3]. In 1941 Drs Baldes and Wood at Mayo clinic brought out tire M-1 maneuver which involved a voluntary muscular tensing effort similar to the Stainforth’s maneuver but with coordinated forced exhalations against a partially closed glottis. The L-1 maneuver was later developed in 1970s at the USAFSAM and is a variation of the M-l maneuver found more useful with less throat irritation for long duration G exposure. This involved straining against a closed glottis. TheL-1 maneuver is taught to the aircrew undergoing HPHC training at IAM.
The present study was done to examine the protection given by AGSM training to aircrew undergoing OPTRAM-F course at IAM. In pursuance of this aim 20 aircrew subjects were given centrifuge runs on two different days. On day I the aircrew were to do straining (whatever they were used to doing in the aircraft) after achieving PLL. On day 2 they were asked to do AGSM after achieving PLL till they attain PLL again. It was hypothesized that there would be a change in the G tolerance of the subjects who were performing AGSM. A well done AGSM is said to provide up to 4G protection [3].
The aircrew are used to perform some amount of straining while pulling G in the aircraft. This does not give enough protection. As seen from the present study the straining which the aircrew are used to, provides 2.1 ±0.7 G protection.
The trained AGSM when performed by the aircrew provided a 3.0±0.1 G protection to the aircrew. This was significant in comparison to straining when the results were analyzed using ANOVA and Tukey’s Multiple Comparison Test.
The AGSM is capable of increasing the G level tolerance by 4G allowing pilots to tolerate 9G - 4G relaxed tolerance, 1 G increases for the anti G suits and 4 G for the AGSM. However, this amount of increase in G tolerance is possible if the pilot is well trained in performing this maneuver, has adequate strength and performs it optimally.
Aircrew from the fighter stream from the different squadrons of the IAF undergo OPTRAM training at IAM, IAF. The training of AGSM imparted at IAM needs to be ingrained in the normal fighter flying. The aircrew need to perform the right AGSM to achieve maximal protection from the ill effects of high G exposure. The squadron aviation medicine specialist is an important member in ensuring that the AGSM training imparted at IAM, IAF is followed in the routine combat sorties at the station level. A good interaction with the aircrew and lectures on the correct technique, advantages and the importance of AGSM needs to be carried out by the aviation medicine specialists.
Conclusion
With a view to study the amount of G protection given to the aircrew by the AGSM (LI maneuver) trained at IAM, IAF. 20 healthy aircrew were given 02 centrifuge exposures (GOR 0.l G/s) on two different days. Day 1 the subjects were to perform straining on achieving PLL while on Day 2 they were to do the AGSM taught to them. A significant difference in the protection afforded by AGSM vs straining was seen. The protection afforded by AGSM was 3.0±0.1 G. Various factors like physical conditioning, amount of muscle tensing, training and practice of AGSM, motivation and mental framework of the aircrew during run predict the effectiveness of a well done AGSM. These factors may be implicated in 3.0±0.1 G protection afforded by the AGSM in comparison to a 4G protection afforded by a well done AGSM.
References
- Biodynamics Sustained acceleration IN In: De Hart RL, ed. Fundamentals of aerospace medicine (2nd ed). Baltimore. MD: Williams & Wilkins; 1996. p. :201-60.
- [Google Scholar]
- Development of Anti G Suits and their limitations. Aviat Space Environ Med. 1987;58:699-706.
- [Google Scholar]




