Translate this page into:
Enhancing Aircrew Protection against Noise Induced Hearing Loss
Abstract
Modern day high performance aircrafts are more powerful, more efficient, and unfortunately, frequently produce high noise levels resulting in Noise Induced Hearing Loss (NIHL) in the Military aircrew. Military pilots are required to perform many flight duties correctly in the midst of many challenges that may affect mission completion as well as aircraft and aircrew safety. Acoustic environment of an aircrew is characterized by several distinctive types of audio signals, speech signals, radio-mediated speech, and aerodynamic and mechanical low frequency noise originating from aircraft and machinery in the vicinity. Perception and localization of relevant sounds and signals, amongst constant background noise, forms a critical part of situational awareness and successful mission completion. NIHL can interfere with the achievement of these objectives. NIHL may also require aircrew to be downgraded from flying duties with the incumbent re-training costs for downgraded personnel and training costs for new/replacement aircrew. As it is not possible to control the source of noise without compromising the efficiency of the engine and aircraft, protecting the aircrew from hazards of excessive noise, and treating NIHL is of extreme importance. In this article we discuss various Personal Hearing Protection Devices and their efficacy, and pharmacological agents for prevention and management of NIHL.
Keywords
Military aircrew
noise induced hearing loss
personal hearing protection devices
pharmacological agents

Introduction
Military pilots are required to perform many flight duties with pinpoint precision in the midst of many challenges that may affect mission completion as well as aircraft and aircrew safety. Among the challenges that interfere with successful mission completion are noise levels, mental workload, communication demand, and individual hearing levels. The design of a next generation high performance aircraft usually begins with a new engine. These engines are generally more powerful, more efficient, and unfortunately, frequently produce high noise levels resulting in Noise Induced Hearing Loss (NIHL). Today’s high performance military aircraft generate noises which typically range from 110 dB to 150 dB.
Normally, the source of the noise cannot be quieted without loss in performance. Therefore use of hearing protection devices (HPD) forms the primary tool to mitigate aviation personnel noise exposures during operations of aircraft. Mechanical hearing protection is essential and effective; however, inherent limitations still allow a significant percentage of permanent hearing loss to occur in aircrew. Hence, pharmacological preventative or rescue agents for NIHL form an important element of a comprehensive approach to maintaining inner ear functional integrity in individuals exposed to noise.
Sources of Noise in Various Aircraft
The majority of the current problems associated with high levels of cockpit noise are generated, essentially, from the post 1960’s aircrafts which need to fly operationally at high speed and low-level, in order to minimize radar detection and decrease exposure time to ground based weapon systems. This has resulted in cockpit noise levels of 115dBto 120dB [1].
High cockpit noise is not exclusive to fast jets. A similar upward trend in cockpit and cabin noise has been exhibited in the military helicopter fleet, Transport and Surveillance aircrafts over the last 30 years.
Pathophysiology of NIHL
NIHL can be Acoustic Trauma or Chronic NIHL [2]. Acoustic trauma refers to a sudden permanent hearing loss caused by a single exposure to an intense sound with sound pressure levels around 130-140 dB resulting in direct mechanical injury to the sensory cells of the cochlea [3]. In contrast, Chronic NIHL occurs gradually over many years of exposure to less intense but continuous noise levels. This process progresses through two phases, temporary threshold shift (TTS) and permanent threshold shift (PTS). TTS is a brief hearing loss that occurs after noise exposure and completely resolves after a period of rest. This is an auditory fatigue and is associated with no or minimal, reversible cell changes. In permanent threshold shift (PTS), there is irreversible hair cell damage.
Cellular Changes in NIHL
Acoustical overstimulation causes mechanical injury of the organ of Corti. especially to outer hair cells. Early noise induced injury involves alterations in hair cell membranes which eventually lead to a failure in the regulation of intracellular ionic composition. A chain of events is set off that involves cell swelling or herniation, increased number of lysosomes and changes in essentially all cellular organelles [3]. The hair cell cilia may become floppy, disordered, splayed, fractured or fused. There is production of reactive oxygen species (ROS) and other free radical molecules in the cochlea, generation of Nitric Oxide, and coinvolvement of Glutamate receptors [4, 5]. Mechanical injury includes microlesions in cell membranes, causing excessive Calcium influx. There is phospholipase A2 activation, superoxide generation by proteolytically activated xanthine oxidase and formation of nitric oxide (NO) and its breakdown products [6].
Glutamate is a major neurotransmitter between the inner hair cell and the afferent cochlear nerveending [7]. Excessive sound stimulation leads to excessive synaptic glutamate concentrations causing overstimulation of glutaminergic receptors (glutamate excitotoxicity), invoking metabolic cascades resulting in cell injury and death. There is mitochondrial injury, inhibition of mitochondrial biogenesis, bioenergetic collapse and loss of redox homeostasis, opening of the mitochondrial permeability transition pore and cell death [8].
Hearing Conservation Progratn
An effective Hearing Conservation Programs has five components:
Assessment of noise levels
Engineering controls
Administrative controls and serial audiometry
Use of personal hearing protection devices (HPD)
Pharmacological Management
National Institute for Occupational Safety and Health (NIOSH, 1998), which is a part of the Center for Disease Control and Prevention (CDC) in the U.S. Department of Health and Human Services, has given guidelines for occupational noise exposure. The sound level and permissible duration of exposure to it, without causing hearing loss, is shown in Table 1.
| Sound Level dBA | Duration of exposure |
|---|---|
| 85 | 8 hours |
| 88 | 4 hours |
| 91 | 2 hours |
| 94 | 1 hour |
| 97 | 30 min |
| 100 | 15min |
| 103 | 7.5 min |
According to these guidelines, an aircrew who is exposed to about 100 dB of sound, should not fly for more than 15 minutes, but flight operations can long much longer than that. Hence Engineering and Administrative control methods cannot be applied to an aircrew. In the following sections personal HPDs, which aim to reduce the noise exposure and effective pharmacological management therapy, which aims to treat and, possibly, prevent NIHL, is discussed.
Personal Hearing Protection Devices
Acoustic environment of an aircrew is constituted by several distinctive types of audio signals, speech signals, radio-mediated speech, aerodynamic and mechanical low frequency noise originating from aircraft and machinery in the vicinity. Perception and localization of such sounds form a critical part of situational awareness. The objective of hearing protection devices in an aircrew is to provide effective hearing protection as well as provide effective communication channels and situational awareness.
Currently, three basic types of personal noise reduction approaches are in use, passive noise reduction, active reduction and a combination of the two [9]. Passive noise reduction systems are earmuffs and earplugs which can be used in isolation. Active noise reduction devices (Electronic Pass through Hearing Protection Devices or EPHPs) are combined with passive HPDs which aim to achieve the above mentioned objectives. They electronically filter environmental noise, permitting only the filtered result to pass through to the listener, with an aim to focus on signals of interest and reduce interference from competing sources.
An EPHP device consists of a pair of conventional, level-independent earplugs or earmuffs, bilateral external microphones to pick up the ambient sound, internal speakers to present these to the ears, and an electronic processing unit which will pass and possibly amplify low-level sounds, reduce high-level continuous sounds using Active noise reduction and block impulsive sounds [10] .The electronic circuit housed within the ear- muffs samples and inverts the incoming waveform and adds it out of phase to the original. A noise- cancellation speaker emits a sound wave with the same amplitude but with inverted phase (antiphase) to the original sound. The waves combine to form a new wave, in a process called interference, and effectively cancel each other out (phase cancellation), thus reducing the volume of the original signal [11].
Conventional HPDs
Conventional HPDs, also known as Level independent or Amplitude insensitive devices, are Ear Plugs and Ear Muffs, which reduce amplitude of all sources without discrimination by same amount regardless of the sound level. Though they can be effective at protecting hearing, but they result in compromised auditory perception, degraded signal detection, reduced speech communication abilities, and diminished situational awareness in an air crew.
Earplugs
Earplugs are available in various types like foam, pre-molded, custom molded, moldable and communication, with attenuation levels ranging from 10 dB to 40 dB [11]. These are effective only when properly inserted and studies have shown that training in the insertion of regular ear plugs improves noise attenuation by 10 dB.
Earplugs are especially useful wnen noise exposure is continuously sustained. The level of attenuation achieved and their communication ability varies with different ear plugs. Foam plugs were found to give higher attenuation than the silicone plug at all frequencies, but particularly at frequencies below 2 kHz [12].
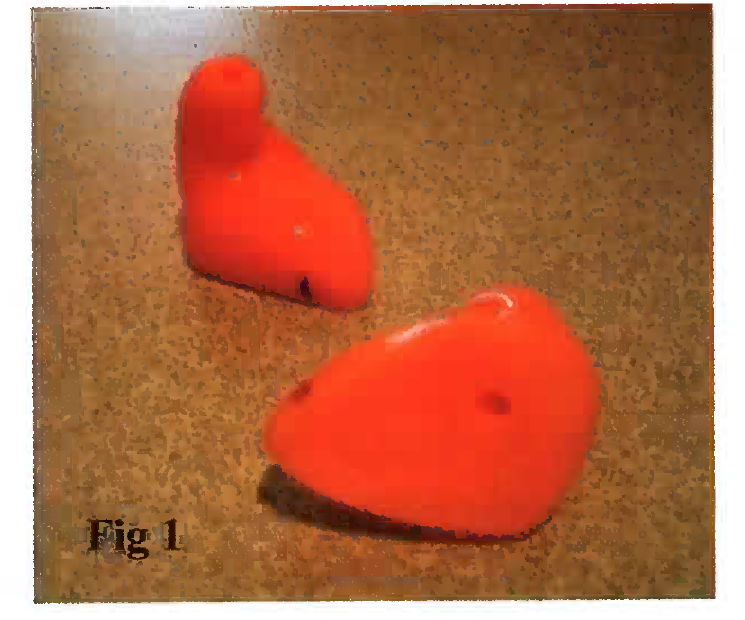
Custom Moulded Earplug
Custom moulded earplugs [Fig 1] are made- to-measure to the individual’s auditory ear canal [13]. They also have an integrated silicone pressure relief tube, which helps to equalize pressure behind the impression and the ear drum. These devices are personally tailored and individually fitted by an experienced operator. Thus they have a personalised physical fit as well as a personalised acoustic fit and are found to perform more consistently than conventional earplugs.
Combat Arms Earplugs (CAE)
CAE is a two-ended, earplug-type hearing protector that was designed to mitigate the noise exposures, while providing minimal reduction of desired signals and speech. It is a preformed, triple- flanged earplug, and its conventional passive end is intended to be worn during hazardous continuous exposures. The other end has a tube through the plug and is intended to be worn when bearing protection is needed against impulsive noise, but when audibility of external sounds is also needed during quiet periods. This sound pathway tube is internally occluded by a thin wafer with an orifice at its center. Sounds that are up to moderately high levels, such as speech communications and signals, can pass through this orifice in relatively unimpeded fashion since their waves exhibit laminar flow in the tube. Thus, in relative quiet environment, signals and speech can be heard through the yellow end of the earplug, while a sharp increase in attenuation occurs at gunshot levels.
Communication Ear Plugs
The communication earplug [Fig 2] was developed by the U.S. Army Aeromedical Research Laboratory at Fort Rucker, Alabama to provide hearing protection by an expanding foam earplug while passing to the ear the clearest speech signal attainable. A miniature transducer and foam earplug are coupled in a unique arrangement to yield a light weight, high quality communications device that can be used alone or in combination with circumaural hearing protection, thus providing the user with excellent sound attenuation and improved speech intelligibility. The foam tip is attached to the transducer using a threaded hollow tube, to provide a pathway that allows sound to travel from the transducer, unimpeded, into the occluded ear canal.
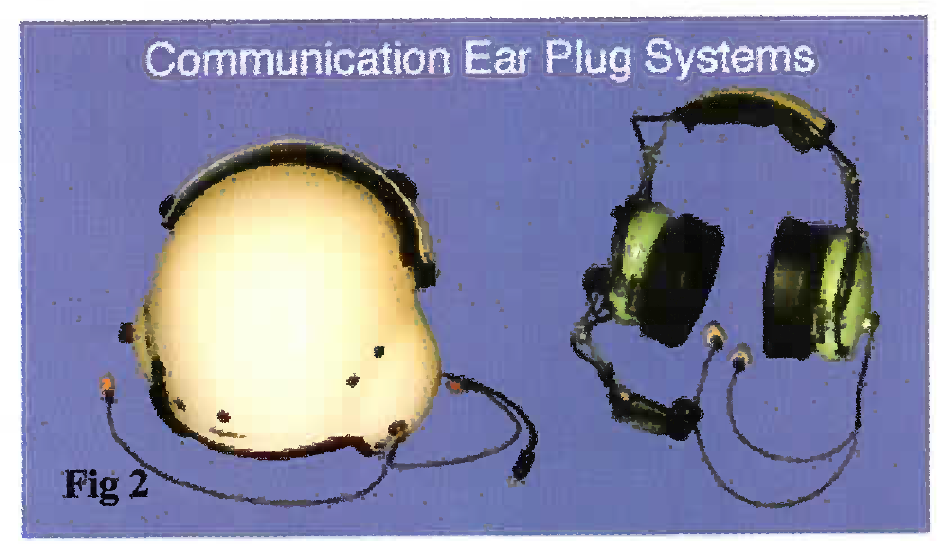
When worn in combination with other hearing protection, communication ear plug reduces noise exposure to minimal levels. Ah crew have reported better noise attenuation, better communication and improved situational awareness with earplugs [14].
Ear Muffs
Ear muffs provide as much attenuation as ear plugs with an additional advantage that they are easy to correctly place and no training is required for their proper insertion [11].'They are especially useful when exposure to noise is relatively intermittent as they are easy to remove and reapply.
Custom Earmuffs
Custom ear muffs were manufactured in an attempt to prevent leaking of acoustic energy at the interface between human head and ear cups. The technique involved the laser scanning of the user’s head. The resulting head contours were then used to fabricate a custom ear cup flange which was attached to a standard high volume (150 cc) ear cup and headband. Custom ear muff attenuation was found to be better than conventional earmuff attenuation [9].
Currently, active ear muffs that are equipped with ANR technology for communication purposes [Fig 3] appear to offer better alternative than conventional ear muffs [11, 15].

Double Rearing Protection
Double hearing protection using custom made communication ear plugs worn under a headset or a helmet appears to be the best. Unlike other HPDs this combination does not interfere with speech intelligibility [16, 17].
Flight Helmets and Noise
The Sound Protection Helmet (SPH-4), which was specifically designed for sound protection in 1970, consisted of a headset mounted in 6 mm thick molded plastic ear cups. It was modified later with a thicker energy absorbing liner to reduce the risk of concussions [18]. Over the years some hearing protection companies have significantly improved passive attenuation in the flight helmets through the innovative use of new materials and structures, which allows the use of existing helmets and require changes to only the headset. Further development of the existing analogue ANR system (through miniaturization of the electronic circuitry), integration of digital ANR techniques and use of Communication Ear plugs [Fig 4]. enhances the sound protective effect of the helmets [19,20], and improves communication and situational awareness in the aircrew.

Communication Enhancement and Protection System (CEPs)
CEP, is designed to control the sound level that arrives at the ear and provide the user with radio communications ability and hearing of external (ambient) sounds via a sound-transmission system, all in a small insert-type earphone that is connected to two separate gain control and power supply/radio control modules. Ambient sounds are attenuated by a compressible foam ear tip, which attaches to the tube of a “hearing enhancement module (HEM)” housing that comprises the insert earphone.
A microphone mounted on the exterior end of each HEM of the CEPS captures ambient sound for processing (through embedded circuitry), and true binaural hearing is provided since the microphone pickup and ambient signal processing are separate for each ear. The processed signal is input to the ear through a miniature loudspeaker inside the HEM from which the signal travels. A boom microphone, which clamps to the helmet, is provided to allow the Air warrior to communicate via radio.
Pharmacological Agents
Inherent limitations of HPD include:
Noise exceeding the protective capabilities of the device
Skull transmission of damaging acoustic energy
Fitting
Compliance issues
Hence pharmacotherapy forms an integral part of hearing conservation programme for aircrew. The ideal pharmacologic agent would specifically address known mechanisms of acoustic injury, be orally administered, be exceptionally safe, be effective and affordable. Though currently such a pharmacological agent is not available, but the ongoing research is promising. Various pharmacological agents and newer developments are discussed in the following sections:
N- Acetyl-L-Cysteine (NAC)
NAC is an anti-oxidant which inhibits lipid peroxidation and scavenges ROS within the cell, indirectly by increasing the intracellular levels of Glutathione (GSH) by acting as a cysteine donor to increase GSH synthesis [21]. It also reduces the level of caspases and glutamate excitotoxicity.
NAC is effective if administered immediately after noise exposure and in the following days. In animal studies, NAC is found to be a safe and effective molecule, given in a dose of 500 mg/kg intra peritoneal, administered immediately after noise exposure and then during the following two days (cumulative dose of 1500 mg/kg). Also, the molecular weight of NAC is low enough to allow it to be transported across the round window membrane, thus creating a possibility of intra- tympanic administration [22]. However, further research concerning the most beneficial methods of administration, the dose of NAC and an eventual association with other compounds is needed in order to offer adequate protection against all components of NIHL.
Acetyl-L-Carnitine (ALCAR)
ALCAR is an endogenous mitochondrial membrane compound .that helps maintain mitochondrial bioenergetics and biogenesis in the face of oxidative stress. If given before and after the noise exposures, it is shown to decrease the amount of hair cell loss and PTS induced by the continuous noise, probably by increasing ATP production, restoring carnitine and cardiolipin levels, enhancing the activity of cytochrome c oxidase, enhancing mitochondrial DNA transcription, restoring the transport of key mitochondrial metabolites, and protecting mitochondrial membrane integrity [23].
The doses in adults of 1.5 to 3 g per day for as long as a year demonstrates that ALCAR is very well tolerated.
D- Methionine (MET)
MET, a derivative of Disulfiram, exerts its otoprotective action by improving cochlear GSH deficiency state. It provides cysteine for synthesis of GSH scavenges free radicals and inhibits the injury-induced GSH efflux from the injured hair cell. MET can rescue individuals from permanent noise- induced hearing loss when initiated 1 h after noise exposure. The hair cell-sparing ability of the MET against NIHL was found to be over 90% in animal studies [23].
Glutamate Antagonists
Glutamate excitotoxicity invokes metabolic cascades resulting in cell injury and death. Glutamate antagonists act through various mechanisms like complete inhibition on interaction with the Glutaminergic receptors (e.g., CGS 19755), direct action at receptor-linked, calcium ion channels (e.g., phencyclidine or MK 801), and interaction with the redox modulatory site of the N-methyl-D-aspartate (NMDA) receptors (DETC-GS) [30].
Carbamethione, a glutamate antagonist and a metabolite of Disulfiram, acts on NMDA receptors and downregulates NMDA receptor activity. This results in reducing presynaptic release of glutamate and also prevents the consequences of glutamate release postsynaptically [30]. Prior application of another broad-spectrum glutamate receptor antagonist Kynurenate can reduce mechanical noise induced ischemic cochlear injury consisting of destruction of dendrites beneath hair cells [23].
Creatine
Creatine prevents noise induced change in ATP homeostasis in the cochlea. This reduces the immediate stress-induced pathophysiology, formation of free radicals and thus prevents cell death. It functions as an energy buffer through creatine kinase, which is abundant in marginal cells of the cochlear striavascularis. Creatine may also contribute to the maintenance of the endocochlear K+ level, thus reducing this immediate effect of noise. Creatine can reduce both temporary (TTS) and permanent (PTS) threshold shifts [24].
Tempol
Tempol is a membrane-permeable radical scavenger that interferes with the formation or the effects of many radicals, thus preventing cell death. Preclinical studies suggest that Tempol may be useful in the therapy of cochlear ischemia- reperfusion injury, shock, and inflammation [24]. Tempol attenuates the PTS only. It has been used to treat humans topically but not systemically, and side effects of oral consumption in humans are currently unknown. Present research is focused on dose response studies for systemic administration as well as direct (cannula-osmotic pump) administration of this agent locally into the scalatympani [23].
Studies till date indicate that with oral administration creatine and tempol can cross the blood-perilymph barrier, reach the tissues of the cochlea and attenuate noise-induced hearing loss. Also, a combined administration of Creatine and Tempol appears to provide more benefit at l6KHz, than Tempol alone [24].
Magnesium
Magnesium has been found to have preventive as well as therapeutic effect on noise trauma [25]. Intracochlear Mg level plays an important role in preventing noise trauma by protecting against impairment of cochlear microcirculation and systemic microcirculatory impairment [26]. It also acts as an NMDA antagonist and reduces intracellular glutamate release. Mg may also contribute to protecting the cochlea against free radicals.
Any kind of Mg therapy in noise trauma should be started as soon as possible after the exposure. In order to improve the therapeutic efficacy, further experimental studies using local application of Mg alone and in combination with another NMDA antagonist or anti-oxidant and free radical scavenger are in progress [26].
Steroids
Glucocorticoids have been widely used in the treatment of idiopathic sudden sensorineural hearing loss in humans for their anti-inflammatory, antioxidant, antiapoptotic and neuroprotective effects. When administrated one hour after the noise exposure, hair cells exhibitless threshold shift and less damage [27] .The activation of the enzyme Na, K-ATPase by corticosteroids maycontribute to restoration of disturbed cellular osmolarity, electrochemical gradients,and neuronal conduction [28]. Corticosteroids act both at the dendritic and the cellular level and directly protect outer hair cells. Transtympanictargeted steroid therapy through a round window microcatheter has shown some hearing improvement in individuals who have not responded to systemic therapy. Apart from avoiding systemic side effects this method achieves higher local concentration of steroids.
Hyperbaric Oxygen Therapy (HBOT)
HBOT aims to repair microcirculation and there is a demonstrable significant decrease in injured cochlear hair cells following HBOT. The improved oxygenation of the inner ear activates cell metabolism and the Sodium- Potassium pump, leading to restoration of the ionic balance and the electrophysiologic functions of the cochlea. HBOT is also capable of causing a reduction in hematocrit and blood viscosity, and this can have a rheologic effect in the cochlear region [29]. Ten once-daily sessions (90 minutes per session) of HBOT at 2.2 ATA, can be delivered in a multipersonchamber.
HBOT can be combined with corticosteroids as coticosteroids induce oxygen consumption to mobilize amino acid for glucogenesis and alter glucose utilisation by oxygen consumingmechanisms, for significantlyimproved functional and morphological recovery.
Antioxidant Gene Therapy
Antioxidant gene therapy is a potential therapeutic strategy to reduce inner ear oxidative stress. Studies have demonstrated that genes delivered to the inner ear can induce functional antioxidant enzymes and can effectively protect hair cells and hearing. The inoculation of the adenoviral vectors is done through a cochleostomy at the base of the cochlea of antioxidant enzymes like catalase, Cu/Zn superoxide dismutase, and Mn superoxide dismutase. The superoxide enzymes protects by dismutating superoxide (02) into the proradical hydrogen peroxide (H202), which in turn is inactivated to oxygen and water by catalase or other H202-removing enzymes such as glutathione peroxidase. Thus it prevents the formation of Superoxide and highly toxic peroxynitrite [30].
As systemic administration of antioxidants is possible, not the first treatment of choice, but further research is in progress to simplify the mode of administration.
Nanomedicine
Nanoparticles can be converted to miniaturized Biosensors by attaching various ligands for early detection of hearing loss. Nanobiotechnology can be used to engineer Noise absorption fillers which can enhance effectiveness of personal hearing protection devices. Nanocapsules can be used for Targeted drug delivery, which allows efficient drug accumulation at target sites, so that sustained and controlled release of drugs at target sites over a period of days or even weeks is possible. Nanoparticles can be used as gene carriers for Gene therapy, thus obviating the need to use viral vectors, thereby avoiding harmful effects of the viruses on human body.
Regenration of Hair Cells
Recent research has shown several promising leads that may overcome the lack of spontaneous regeneration of hair cells in organ of corti in the mammals. Studies in animals that spontaneously regenerate hair cells, such as birds and fish, are unveiling important molecules needed to reach this goal. Attempts are made to stimulate existing stemlike cells in the human inner ear to regenerate hair cells, by delivering molecules that stimulate new hair cell production. A second approach is to transplant stem-like cells into the damaged ear that can give rise to new hair cells. Gene therapy, stem cells therapy and possible integration of both these approaches, may in future provide a biological cure for deafness. For example, mammals with an absent P27 gene display intracochlear cellular differentiation and the appearance of new hair-like cells after injury. Gene therapy with Atohl has resulted in patchy prototype hair cell formation in vivo and in vitro. Other genes like GDN, HGF, BDNF, NTF-3, EGFP and GJB2 are being currently researched. The ability to stably and specifically target damaged tissue safely with both exogenous stem cells and the necessary genes is the final step necessary for hearing loss restoration.
Condition
The high noise levels that some aircrew are subjected to will, without adequate protection, cause permanent hearing damage which, in turn, will require aircrew to be downgraded from flying duties with the incumbent re-training costs for downgraded personnel and training costs for new/replacement aircrew. To date, of all studies aimed at the prevention of noise-induced hearing loss, none propose that it is entirely preventable, other than by avoiding the exposure, which, in an aircrew, is not feasible. Technological advancements in personal hearing protection devices, such as use of ANR technology, miniaturising and digitalizing the electronic circuitry in ANR Systems, communication ear plugs along with sound attenuating flight helmets, are some of the methods which provide protection against NIHL. But still military surveys have shown that even with the very best hearing protection, NIHL does occur. Hence besides hearing protection, there is a need for further research for developing an effective pharmacological agent for management of NIHL, preferably multi-drug therapy, which will be able to address all metabolically induced and mechanically induced stress-related events.
References
- Defining the Cockpit Noise Hazard, Aircrew Hearing Damage Risk and the Benefits Active Noise Reduction Headsets Can Provide RTQ-EN-HFM-111 Lecture Series on “Personal Hearing Protection including Active Noise Reduction”, held in Warsaw, Poland, 25-26, Oct, 2004, Belgium, Brussels. 2004 Oct 28-29:5-24.
- [Google Scholar]
- Acoustic damage of the cochlea. A scanning and transmission electron microscopic observation. Arch Otolaryngol. 1971;94:294-305.
- [Google Scholar]
- The emergence of free radicals after acoustic trauma and strial blood flow. ActaOtolaryngolSuppl (Stockh). 1995;519:87-92.
- [Google Scholar]
- Early elevation of cochlear reactive oxygen species following noise exposure. AudiolNeuroOtoll. ;999:229-236.
- [Google Scholar]
- Glutamate is the afferent neurotransmitter in the human cochlea. ActaOtolaryngol (Stockh). 2000;120:359-362.
- [Google Scholar]
- Passive Hearing Protection Systems and Their Performance. Paper presented at the RTO HFM Lecture Series on “Personal Hearing Protection including Active Noise Reduction. ”RTO-EN-HFM- 111. Paper 2:21-2.:13-2.
- [Google Scholar]
- Protection efficiency of hearing protectors against military noise from handheld weapons and vehicles. Noise Health. 2005;7:11-20.
- [Google Scholar]
- A Comparison Study of Foam versus Custom Silicone Earplugs Used as Part of an Intelligent Electronic Hearing Protector System. International Journal of Acoustics and Vibration. 2010;15:151-155.
- [Google Scholar]
- Communication earplug and active noise reduction: Hearing protection technologies for Air Warrior. U.S. Army Aviation Digest 1995 March/April:20-21.
- [Google Scholar]
- Speech understanding in noise with integrated in-ear and muff-style hearing protection systems. Noise and Health. 2011;13(55):378-384.
- [Google Scholar]
- Double hearing protection and speech intelligibility-room for improvement. Aviat Space Environ Med. 2001;72(4):400-4.
- [Google Scholar]
- Sound Attenuation from Earmuffs and Earplugs in Combination: Maximum Benefits vs Missed Information. ” Aviat. Space Env. Med. 2006;77(9):899-904.
- [Google Scholar]
- SPH-4 Aircrew Helmet Impact Protection Improvements 1970-1990. USAARL Report Feb 1991:91-11.
- [Google Scholar]
- Qualitative evaluation of aircrew helmet passive noise reduction and the communication earplug for tactical aviation. Proceedings of the human factors and ergonomics society annual meeting for tactical aviation. 2001;45:166-170.
- [Google Scholar]
- Balancing speech intelligibility versus sound exposure in selection of personal hearing protection equipment for Chinook aircrews. In: Aviat Space Environ Med. Vol 72. 2001. p. :1037-44.
- [Google Scholar]
- Protection from noise-induced lipid peroxidation and hair cell loss in the cochlea. Brain Res. 2003;2:265-73.
- [Google Scholar]
- Candidate thesis Enhancing Noise-Induced Hearing Loss Defenses. Laryngoscope. 2002;112:1515-1532.
- [Google Scholar]
- Excitotoxicity and repair of cochlear synapses after noise-trauma induced hearing loss. Neuroreport. l998;9:2109-2114.
- [Google Scholar]
- Creatine and Tempol attenuate noise-induced hearing loss. Brain Res. 2007;1148:83-89.
- [Google Scholar]
- Therapeutic effect of magnesium on noise-induced hearing loss. Noise Health. 2001;3:79-84.
- [Google Scholar]
- Long-term administration of magnesium after acoustic trauma caused by gunshot noise in guinea pigs. Hearing Research. 2009;247(2):137-145.
- [Google Scholar]
- Treatment of Noise-Induced Hearing Loss. International Congress Report.
- Successful treatment of noise-induced cochlear ischemia, hypoxia, and hearing loss. Ann. N. Y. Acad. Sci. 1999;884:233-248.
- [Google Scholar]
- The Effect of Hyperbaric Oxygen Therapy in Comparison to Conventional or Placebo Therapy or No Treatment in Idiopathic Sudden Hearing Loss, Acoustic Trauma, Noise-Induced Hearing Loss and Tinnitus. Advances in Otorhinolaryngology. 1998;54:86-99.
- [Google Scholar]
- Antioxidant Gene Therapy Can Protect Hearing and Hair Cells from Ototoxicity. Molecular Therapy. 2004;9:173-181.
- [Google Scholar]
- Regeneration of hair cells; making sense of all the noise. pharaceuticals. 2011;4:848-879.
- [Google Scholar]




