Translate this page into:
Controlled flight into terrain during visual meterological conditions (VMC) is a reality - A case report
Abstract
A 26 year old fully Ops fighter pilot with a total of 600 flying hours. 300 hours on type and 246 hours solo was detailed to fly in a 4 aircraft formation for a Lay Down Attack (LDA). The mission got airborne at 0600 h in clear weather. During the third run over the target and in the base leg the aircraft gradually descended, in c controlled manner into the ground, from a height of 50 meters. The pilot was fatally injured. There was no evidence of aircraft malfunction or pilot incapacitation prior to the fatal event. Controlled flight into terrain during Instrument Metrological Conditions (IMC) is well documented, but what caused this controlled flight in to terrain during Visual Metrological Conditions (VMC) ? Was the past flying history connected with the recent? The case report brings out the salient features which could have led to the accident and is discussed in conjunction with Loss of Situational Awareness (LSA) and Human error-not necessarily pilot error; Remedial action from the Aeromedical point of view is suggested.
Keywords
Loss of Situational Awareness
Controlled flight
Human error

The Mission: A 26 year old fully Ops fighter pilot was authorised to fly as No. 2. in a 4 aircraft (ac) LDA bomb strike over the Range. The navigation was planned at 150 meters (mtrs) and thereafter the formation was to “run in” attack formation, with each member trailing the preceding member by a * distance of 3 Kms. The members were briefed to descend to the weapon release height of 50 mts, only after visually acquiring the target and after having done the final alignment. The formation ran in as briefed but only the leader dropped the bomb in the first run. The No. 2 dropped one bomb in his second pass. The release height was reported to be 70 mtrs and the bomb had undershot the target by 100 mtrs. During the next circuit the No. 2 was last seen in the attack direction by the No. 3 who was following. Subsequently a huge ball of fire was seen in the attack direction, later identified as the No. 2's aircraft.
The Machine : The Aircraft (ac) was fully serviceable and had no history of malfunction pertaining to the engine, control systems, auto-pilot and hydraulic system. The ac had flown two sorties in day and two sorties during night on the day prior to the accident. The ac was declared serviceable for flying and properly loaded with weapons for the mission.
The Man : The pilot was assessed as “Average” to “High Average” during his Basic and Advanced training. His performance in armament phase was “Above Average”. In his MiG Operational Flying Training his performance was “Average Plus”. He had a total flying experience of 594:55 hours, was declared Fully Ops four months prior to the accident and had a “White” rating in Instrument Flying. He had a break in flying of about two and a half months due to a ground-training course and due to leave. On his return from leave, about 2 days prior to the accident, he flew a dual check with the Flight commander and this sortie was assessed as “Average”. The day prior to the fateful mission, he flew two handling sorties and one PI (Practice Interception), sortie, all solo.
He was a person of moderate habits, smoked occasionally and consumed alcohol occasionally. During his last Annual Medical Examination in March 98 he was found to be in Category A1G1 and also found to be medically fit for the sortie. There was no record of illness prior to the accident and he did not show any adverse features during his preflight medical.
Findings
The Terrain: The terrain over the range was featureless, with gently undulating sand dunes, covered occasionally by small shrubs. The weather was clear with no dust or early morning haze, thereby making visibility good. The target was clearly marked out and was visible from the time the ac turned for the attack. The light conditions were adequate as the sun was already up and was not in the line of sight of the pilot.
The Crash : The sortie was correctly authorized and was the first sortie of the day for the pilot. The ac was serviceable pre-fight. In-flight serviceability was confirmed by the SAARP analysis (Fig. 1). However, the last 5-10 seconds of the film were exposed when the ac crashed and was not available for analysis. In the SAARP analysis the altitude line showed a gradual upward movement indicating a gradual descent. The air speed had reduced from 800 kmph to 780 kmph. Vg showed an increase to +2.6g during turning of the ac and thereafter to +lg as the ac levelled out. The RPM showed build up to 100% and thereafter kept steady between 95-98%. No change in the Hg line was seen. The Stab deflection was between -6 to 4.8, which was considered normal with respect to the attitude of the ac. The jet nozzle was clearly seen to the end. Neither did the pilot report any abnormally or emergency on R/T. The flight parameters also revealed that the pilot's flying was steady. His turn onto finals during the first two circuits was done gradually, however in the third circuit this turn was done abruptly, albeit smoothly. From the ac impact points and spread of the wreckage it appeared that the ac gradually descended at a shallow angle and at an airspeed of about 780 km/hr before it impacted with the ground. After the impact, the ac disintegrated into small pieces and the wreckage spread over 800 mtrs linearly (Fig 2). The sideways spread was 50m to the right and 30m to the left. The cockpit was smashed and lying about 700m from the initial impact. The radio altimeter critical altitude height selector switch was not located. The body was found strapped to the seat, in the cockpit, in a slightly charred condition, with the head and left forearm missing. There was no evidence of in-flight incapacitation. Bird strike could not be ruled out. The post-mortem was not contributory.
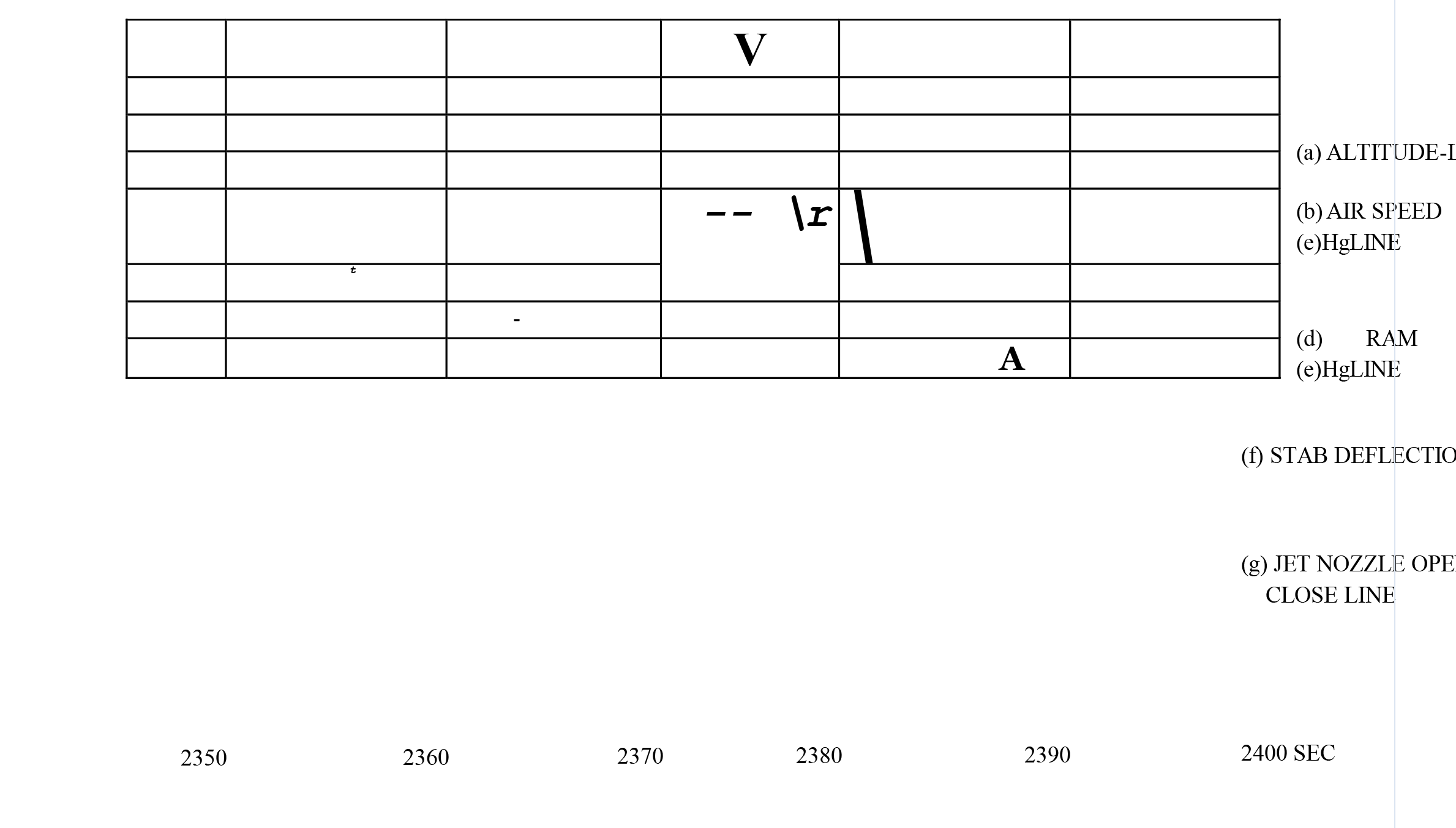
- Saarp anal ysis showing the flight parameters as recorded during the last 50 seconds of flight
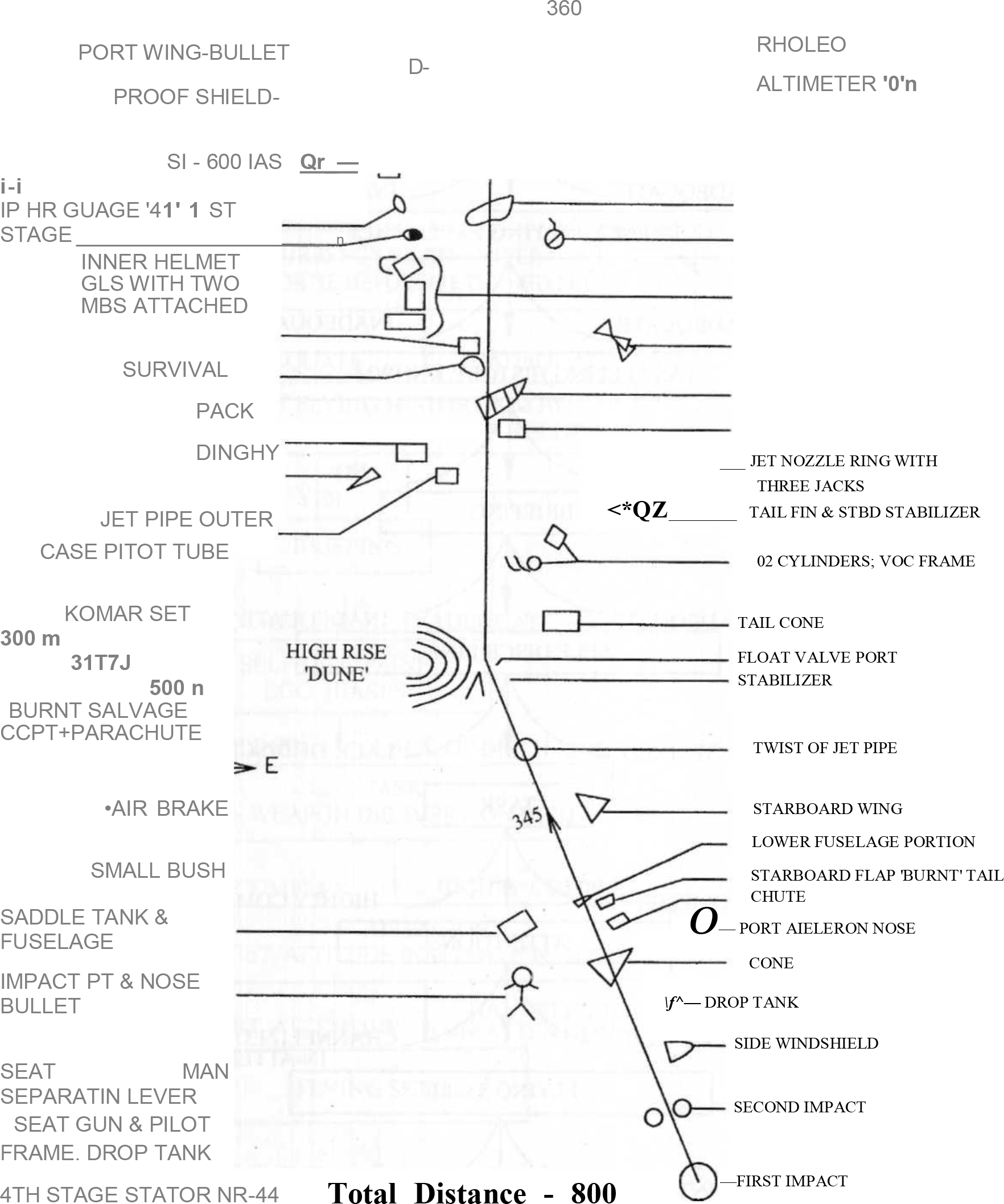
- Fig. 2:
The Man : The pilot came to his last squadron with a slightly checkered flying history. He had been warned once for flying indiscipline, which is not unusual considering his keenness to fly, as was brought out in the “Blue Book”. Also on record is the fact that his weapon delivery was above the average and he had secured a Trophy for the same. On arrival at his new location and on his first flight with his Commanding Officer (CO), he was cautioned against “Channelised attention” and was found to be “lacking in Situational Awareness”. With the result he was given additional sorties before he was allowed to begin the Training Syllabus for his Ops Status. Three months later when assessed by the new CO, he was again warned for “Tunneling of Attention” and made aware of its consequences. The second warning was given to drive home the point and it was felt that in due course, if the pilot did not have any long break in flying, the problem would be overcome. This fact was borne out in that, the Blue Book has no longer any mention of this trait for the next seven months of flying. He had last flown an LDA bomb attack six months previously and never in a four ac formation.
He had returned from leave quite happy and in a good frame of mind. His last few evenings were spent in the company of friends where he actively took interest in the proceedings.
Discussion
A healthy fully Ops pilot and a healthy aircraft no longer exist.
Why did it happen ?
To try and answer this there are many pertinent points
The Range: A featureless terrain, but a familiar one.
The LDA sortie : The pilot had last done a LDA bomb attack six months ago-a fact that was not known to the leader of the mission.
The Radio altimeter warning : Was it ignored or was it switched off? The fact will remain unresolved.
-
The Pilot:
Keenness to prove : He could not take part in a recent Fire Power Demonstration (FPD), even though he had trained for it. He could not hit the target on his first two runs. Thus may have affected his ego as he had a Trophy in the Gunnery Meet and wad considered good enough to take part in the FPD.
Tendency for Inattention: In circuits and also for not concentrating on all that is happening in the cockpit. In the past an incident occurred when he strayed to the side of the Taxi track, when taxying back after a sortie.
Tendency for Channelized Attention : Paying attention to only one parameter at the cost of others.
Tendency for Distraction. Sudden roll out on the third run. Distracted by the sudden thought that he has only two more bombs in which to score a direct hit.
Though the eventual factor is the pilot it would be more appropriate to label the problem as one of Human Error as there were many issues which played their role in the chain of events which eventually led to the occurence of the accident (Fig. 3). However, the actual accident may be attributed to a Loss of Situational Awareness (LSA).
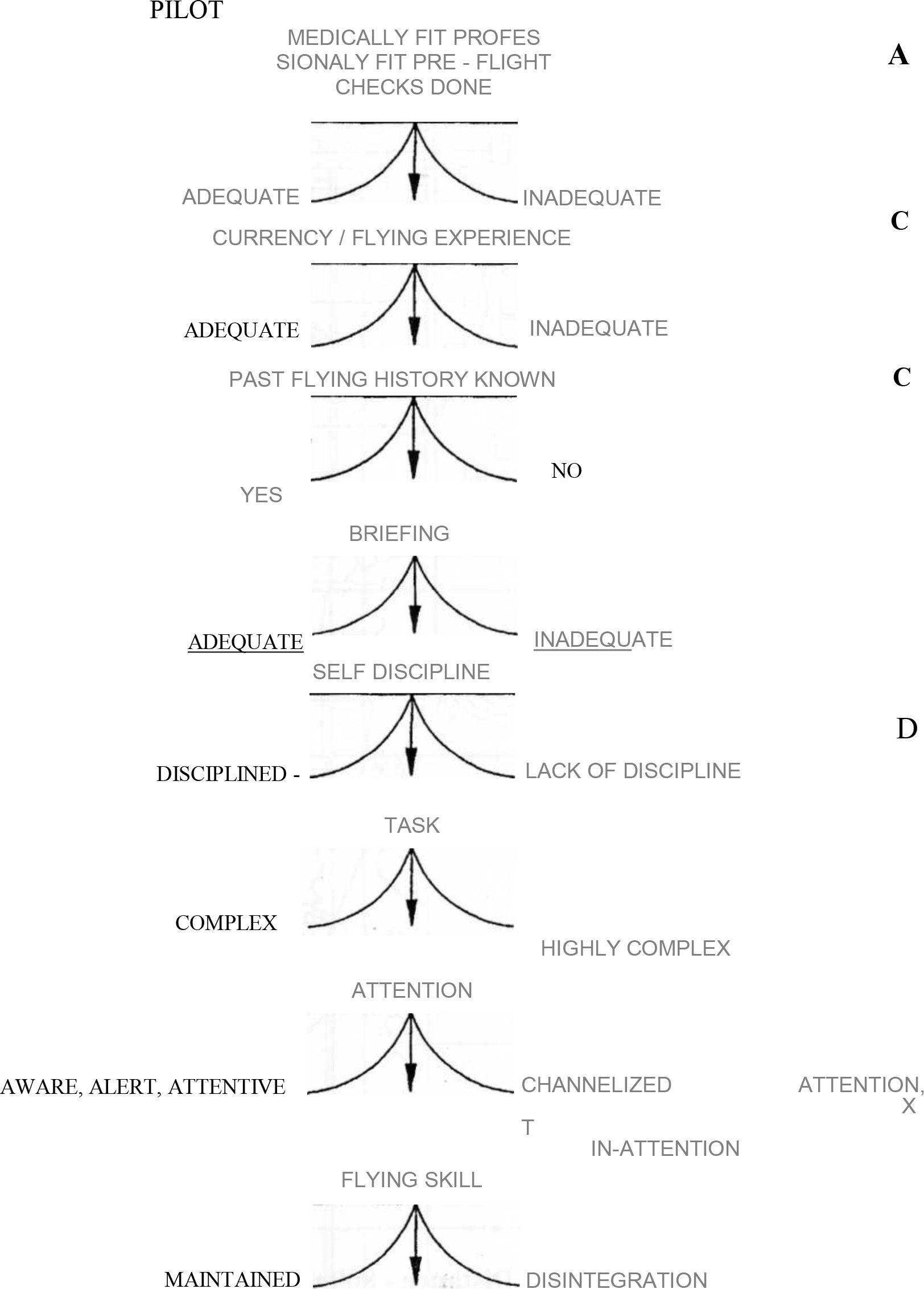
- Aero-medical considerations in the causation of the accident
Situational Awareness (SA) [1] is defined as the “pilot's continuous perception of self and aircraft in relation to the dynamic environment of flight, threats and mission and the ability to forecast, then execute tasks based on that perception”. LSA and Spatial Disorientation (SD) are often used synonymously. However, the definition is quite different from that Spatial Disorientation and the limitations of the current SD definition [2] and its proponents and deponents has been already addressed [3]. The overlap between LSA and SD is always present, as in all cases of LSA there has been a secondary loss of Spatial Orientation and in all cases of SD there has been Loss of Attitude Situational Awareness. Subsets of SA as noted by Vandeerbeek describe operational situations and form elements of Global SA [4]. At any given time one or more of these subsets may get degraded.
In a study on re-categorisation of F-16 Class-A mishaps, of the 65 mishaps over a 8 year period 56 were attributed to degradation of SA. The same study revealed that of the 28 LSA/SDO mishaps, all of which were fatal, 6 occurred during VMC with a distinct horizon while 22 occurred in a degraded visual environment. The authors also brought in the concept of an SA Umbrella (SARBELLA) which takes into account factors which degrade SA and those which help retaining awareness with time and additional information add stability to the SA platform [4].
In most cases of LSA, it is found that degraded tactical awareness has been instrumental in the causation of the accident. Task saturation, channelized attention, distraction and task misprioritization are the other factors which lead to degraded Tactical awareness and LSA. Psychological awareness also plays a part in LSA, as the pilot trying to gain an advantage disregards aircraft parameters. Lyons et al found that when Sensory/ Perceptual and SA factors were coded, 10/13 accidents had channelized attention (inadequate cockpit attention) while misperception of position, vestibular illusions and distraction was seen 5/13 suggesting an overlap of various factors [5].
Therefore taking into account the above studies and translating them into the flow diagram given earlier, a reconstruction of the factors that could have led to the accident are given in Fig. 4.
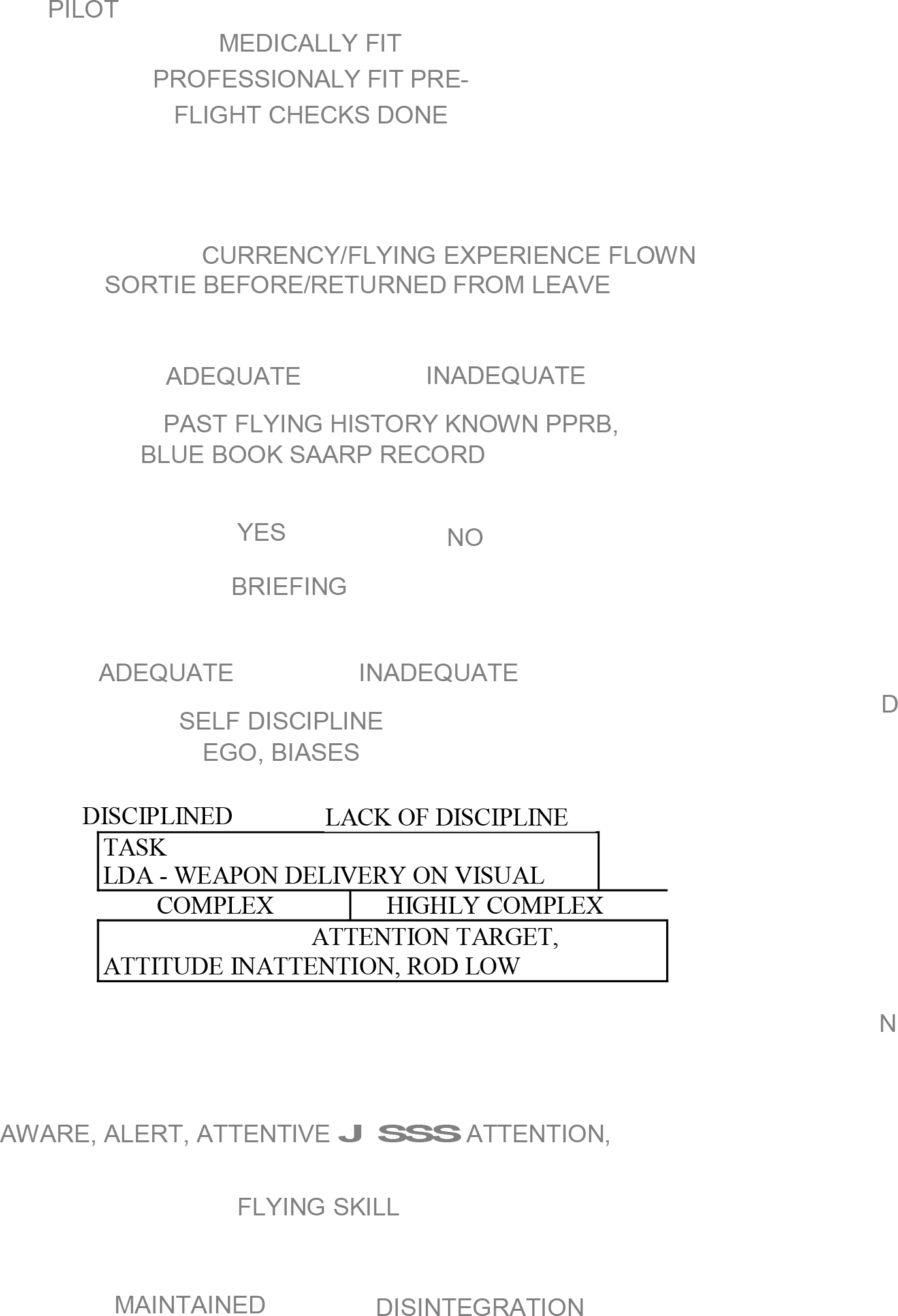
- Aero-medical considerations in the causation of the accident in conjuction with LSA & human error
Could this accident have been prevented? In hindsight preventive measures could have been taken had the concerned people been aware. The lacunae in the system are not within the purview of the article. From the Aeromedical point of view the following preventive measures are outlined for cases where LSA is detected during a pilots flying career.
Simulator Flying: Full motion simulator with the capability of simulating live targets with the aid of computer graphics. During such flying the pilot in question should be put through situations that bring out the traits noticed by his superiors.
Team Analysis : Team visualizes components from all aspects of the flying Environment i.e., Aircrew, Aeromedical Specialists, Psychologist, Fighter Controllers.
Desensitzation: To be done in two phases. The first phase is the ground phase while the second phase will take place in a Training establishment or at the Unit level. The idea of desensitzation is to improve attention skill and thereby SA. Critical versus non critical tasks are identified before take-off and task execution monitored. “The overall impact will be heightened awareness skills with a reduction in aircrew error rate”. [4]
Conclusion
A fully Ops pilot, who was detailed for an LDA bomb attack lost his life when a controlled flight into terrain resulted in collision with the ground. He had a tendency for channelized attention and inadequate cockpit attention. His inability to score a direct hit during the first two passes probably resulted in his inattention to other cockpit parameters and therefore resulted in the accident. It is important to recognize the traits and provide a means of desensitizing such individuals with Simulator flying. Aeromedical and Neuropsychological testing would help prevent such problems in the future.
References
- Situational Awareness. Papers and annotated Bibliography. Tech Reprot No. A/CF-TR-1994-0085
- [Google Scholar]
- An operational Definition for Spatial Disorientation. Aviat Space and Environ Med. 1994;66:1153-5.
- [Google Scholar]
- In defense of traditional view of spatial disorientation and loss of situational awareness. Aviat Space and Environ Med. 1995;66:1103-6.
- [Google Scholar]
- Human Factors Causes and Management Strategies in US Air Force F-16 Mishaps 1984-Present 1993 AGARD-532. :22-1.
- [Google Scholar]
- Epidemiology of United States Air Force Spatial Disorientation accident 1993 AGARD-532. :31-1.:11-1.
- [Google Scholar]




