Translate this page into:
Centrifuge training vis-a-vis G-LOC incidents - an update
Abstract
G-induced loss of consciousness (GLOC) is an area of major research and operational interest. With aircrafts sustaining 7 G or more, use of only the anti-G suit is inadequate. Hence, additional protection in the form of anti-G straining man oeuvre (AGSM) becomes a necessity. Centrifuge training is an ideal method to teach an aircrew the correct technique of performing AGSM to increase their G-tolerance and prevent accidents due to in-flight G-LOC. High-G centrifuge training for the fighter pilots in India began in Mar 1991 at the Institute of Aerospace Medicine (IAM), Indian Air Force (IAF). Presently the course is of two weeks duration and known as Advanced Fighter Aircrew Indoctrination Course (AFAIC). It comprises didactic lectures and centrifuge training. The centrifuge training consists of rapid onset runs (ROR), gradual onset runs (GOR) and simulated aerial combat man oeuvre (SACM). In last ten years, i.e. from Mar 91 to Mar 2001, over 415 pilots have been trained. The minimum standard for the course is 7 G for 15 seconds, which is an accepted norm throughout the world. With training, the tolerance of pilots improved from mean figures of 4.2 G relaxed tolerance to 8.87 G straining tolerance for rapid onset runs (ROR) and from 5.01 G relaxed tolerance to 7.9 G straining tolerance for GOR runs. Mean simulated air combat man oeuvre (SACM) tolerance was found to be 179.2 seconds. The incidence of G-LOC was 34.69% in the aircrew trained which was reportedly higher than in other air forces (10-24 %). The present study also includes period from 1998-2001 separately. Earlier studies (1994, 1997) have been compared and total experience of one decade has been included in the current study.
Keywords
Centrifuge
High G training
High sustained G
G-LOC
and AGSM

G-LOC is the most dreaded problem in acceleration physiology and initially it was reported as faintness in the air. The modern generation fighter aircrafts with continually increasing acceleration capabilities have put increased G-loads on every pilot. Hence, G-LOC has become an ever-present threat in fighter flying. A mismatch of the pilot's G-tolerance with the G-envelope capability of the aircraft may result in pilot incapacitation, mission compromise, loss of aircraft and loss of life. Everyone has a G- tolerance limit, both in terms of peak G (G level) and G-duration. Pulling high G is inherent in flying high performance aircraft. Hence, occurrence of G-LOC cannot be eliminated but can only be prevented by taking better protective action. Several protective strategies to increase G tolerance are in vogue and they have contributed in increasing the G tolerance of pilots and thereby have played a significant role in bridging the gap between the capabilities of aircraft and human capacity. One of the strategies adopted by various countries is training their fighter pilots in a controlled and safe environment of a centrifuge. North Atlantic Treaty Organization (NATO) air forces, including the USAF, have centrifuge-training programs in place [1]. One of the important results of high-G research is the demonstration that subjects could be trained to tolerate high-G loads for prolonged periods (9-G up to 45 sec) in a human centrifuge by an optimally effective anti-G straining man oeuvre (AGSM) [1]. The centrifuge is an ideal ground based simulator where lessons can be learnt, a critical evaluation of a pilot's AGSM can be made and proper technique be taught.
The high performance aircraft that are currently operational in IAF (MIG-29, MIRAGE-2000 and SU-30) impose high requirements on the G-tolerance of the aircrew and resulted in the need to continually enhance the G- tolerance capability of each and every fighter pilot. Centrifuges generate rapid onsets and sustained G-forces, typical for those of modern high-performance fighter aircraft. In IAF, centrifuge training has been introduced from Mar 1991 and is being regularly conducted to minimize possible attrition of our aircraft and aircrew due to in-flight G-LOC. During this course the aircrews are given didactic lectures, centrifuge training and also training on physical conditioning. Main emphasis during this training is to teach an aircrew the correct technique of performing AGSM. Our earlier experiences have been compared with the findings of the present study [2, 3, and 4].
The use of muscular tensing and increasing the intra-thoracic pressure by pilots to increase their arterial pressure (Pa) that results in an increase in their G-level tolerance originated in France in about 1924. There are four different methods of doing AGSM. They are Ml man oeuvre, LI man oeuvre, Hook man oeuvre and Qi-Gong man oeuvre. Dr Blades and Dr Wood of Mayo Clinic, in 1941, described the Ml man oeuvre, which consists of voluntary muscular tensing effort, but with coordinated forced exhalations against a partially closed glottis. This significantly increased G-level tolerance. The LI man oeuvre was developed in the late 1970's at United States Air Force School of Aviation Medicine (USAFSAM) and is a variation of the Ml that has less throat irritation during the performance. In the LI, the forced exhalations are against a completely closed glottis. These man oeuvres, together with other modifications, are now simply called anti-G straining man oeuvres (AGSM) [5]. All man oeuvres give an average of 3.5 to 4G protection if performed correctly. LI version is taught in IAM.
Materials and Method
The subjects are the Indian Air Force fighter pilots who undergo high-G training in the department of acceleration physiology. A total of 415 pilots have been trained at IAM till Mar 2001. Only male fighter pilots were trained, as IAF has no female fighter pilots. The high-G centrifuge-training course, which is renamed presently as Advanced Fighter Aircrew Indoctrination Course (AFAIC), is conducted at IAM for a period of two weeks. The content of the course is given in Table 1. Table 2 shows the total number and different types of runs given in the whole course schedule.
| SI. No. | Content |
|---|---|
| 1. | High G Centrifuge training |
| 2. | Spatial Disorientation training |
| 3. | High altitude Physiology training |
| 4. | Human Physiology Indoctrination |
| 5. | Human Factors Indoctrination |
| 6. | Indoctrination to Human Psychology |
| 7. | Indoctrination to Aviation Ophthalmology and Otolaryngology |
| 8. | Physical conditioning programme |
| Type of run | Rate of onset G/sec Xt |
PeakG |
Rate of offset G/sec <U' | |
|---|---|---|---|---|
| Magnitude | Duration | |||
| Warm-up | 05 | 25 | 15 sec | 0.2 |
| GOR | 0.1 | 9.0 | 2 sec | 1.0 |
| R0R1 | 1.0 | 4.0 | 15 sec | 1.0 |
| R0R2 | 1.0 | 5.0 | 30 sec | 1.0 |
| ROR3 | 1.0 | 6.0 | 30 sec | 1.0 |
| R0R4 | 1.0 | 7.0 | 15 sec | 1.0 |
| R0R5 | 1.0 | 8.0 | 10 sec | 1.0 |
| R0R6 | 1.0 | 9.0 | 5 sec | 1.0 |
| SACM | 1.0 | [4&8Galtfor 15&10sec] | 300sec (max) | 1.0 |
| SACM &PBG | 1.0 | [4&8G alt for 15&10sec] | 300sec (max) | 1.0 |
| SD Run | 0.5 | 2Gfor | 60sec | 1.0 |
During the training a certain percentage of pilot population suffers from inadvertent G-LOC. An emergency switch decelerates the centrifuge and an audio alarm is activated. The time from the loss of consciousness to the time of either lifting of head or opening of eyes is considered as absolute incapacitation period. The time from lifting of head to killing of the audio alarm by the pilot is considered as relative incapacitation period. During recovery period many pilots do have myoclonic jerks or dream state, and are categorised as Type-II G-LOC. Others who do not have such sign or symptoms are categorised as Type-I. The period of incapacitation varies with the type of run and also with the presence or absence of signs or symptoms.
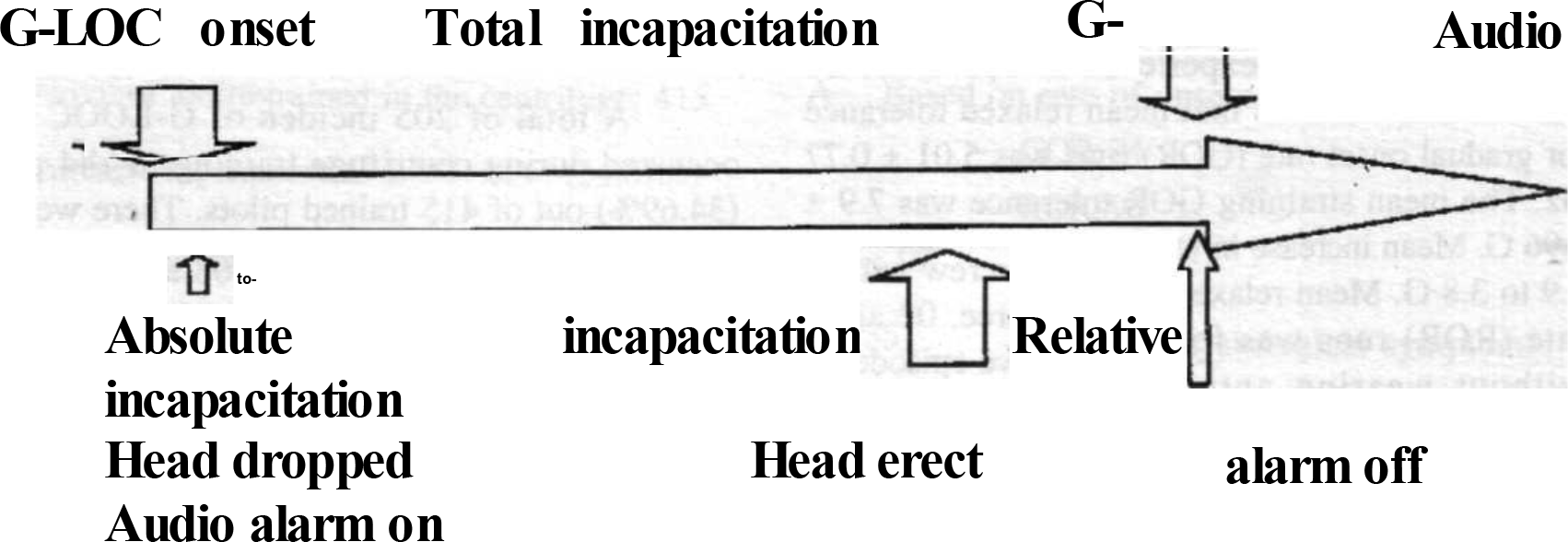
- Fig 1
Results
All parameters mentioned below are with upright The subject data and type of aircraft flown are seat configuration as used by IAF pilots in aircraft. mentioned in Tables 3 & 4.
| SI. No. | Parameter | Range | Mean |
|---|---|---|---|
| 1. | Age(yrs) | 21-35 | 25.7 ± 1.84 |
| 2. | Weight (kg) | 50-90 | 66.26 + 7.35 |
| 3. | Height (cm) | 162.5-190 | 173.67 ± 8.71 |
| 4. | Flying Hrs | 253 - 2680 | 600 + 307.24 |
| SI. No. | Type of aircraft | No. of pilots |
|---|---|---|
| Mirage-2000 | 21 | |
| 2. | MIG-29 | 49 |
| 3. | MIG-=27 | 32 |
| 4 | MG-25 | 01 |
| 5. | MIG-23 | a |
| 6. | MIG-21 | 252 |
| 7. | Jaguar | 23 |
| 8. | Sea Harrier | 04 |
| 9. | Others | 14 |
| Total: | 415 |
The mean age of the subjects was 25 yrs with average flying experience of 600 ± 307.24 hours. Table-5 shows that mean relaxed tolerance for gradual onset rate (GOR) runs was 5.01 ± 0.77 Gz. The mean straining GOR tolerance was 7.9 ± 0.96 G. Mean increase in tolerance with AGSM was 2.9 to 3.8 G. Mean relaxed tolerance to rapid onset rate (ROR) runs was found to be 4.2 ± 0.47 G without wearing anti-G suit, using 52°-56° peripheral light loss (PLL) as the endpoint. Straining tolerance with anti-G suit for rapid onset runs (ROR) was 8.87 G with PLL/CLL/G-LOC as endpoint. Percentage of pilots who have successfully completed straining ROR tolerance for 7 G, 8 G and 9 G are 98.8%, 97.13% and 90.45% respectively. All but 05 pilots could complete the minimum stipulated 7 Gz for 15 sec by the end of the course. 03 of them with low G tolerance and one with a simulator sickness as well were disqualified. 02 were asked to repeat the course after 6 months. 375 (90.45%) aircrew successfully completed 9 Gz for 5 sec, 403 (97.13%) could sustain 8 Gz for 10 sec. and 410 (98.8%) had sustained 7 G for 15 seconds. Mean duration of SACM tolerance was 179.2 sec. Comparative values of US Air Force are given in the same table.
| Parameter | IAF | USAF | P value |
|---|---|---|---|
| Relaxed GOR-tol | 5.01G+0.77 | 5.17G+0.94 | <0.01 |
| Straining GOR-tol | 7.9G±0.96 | 8.32G+0.82 | <0.01 |
| 9 Gz during GOR | 12.5% | 40.8% | |
| Relaxed ROR-tol | 4.27G+0.47 | 4.1 Gz+0.7 | <0.01 |
| Straining 7Gz ROR | 98.8% | - | |
| Straining 8Gz ROR | 97.13 | 99.8% | |
| Straining 9Gz ROR | 90.45% | 94% | |
| Average SACM-tol | 179.2sec | 170sec | <0.01 |
| G-LOC incidence | 34.69% | 9% | <0.01 |
| Course duration | 12 days | 01 day | |
| No. of runs/subject | 30.5 | 05 |
Incidents of G-LOC
A total of 205 incidents of G-LOC have occurred during centrifuge training in 144 pilots (34.69%) out of 415 trained pilots. There were 98 aircrew with single, 35 with two, 08 aircrew with three, 02 aircrew with four and one aircrew with five episodes of G-LOC. The G-LOC data is given in Table 6. Table 7 shows the distribution of the total number of G-LOC cases in different run profiles. The number of G-LOC cases during GOR, ROR and SACM profiles are 24, 96 and 24 respectively. The period of incapacitation in different run profiles are given in Table 8. Table 9 shows distribution of G-LOC cases during ROR runs. Period of incapacitation versus type of G-LOC (Type-I & II) are given in Table 10. Table 11 gives comparison of results of previous two studies in IAM with the present study. Table 12 shows the period of incapacitation in different types of run for 52 cases of G-LOC occurred between Jan 1998 to Mar 2001 out of 154 trained. Table 13 shows that percentage of G-LOC cases amongst those who have done Stage-IIA course is 20% only, in comparison to 37% amongst those who have not done Stage-IIA course.
| 1. | No. of aircrew trained in the centrifuge: 415 |
| 2. | Aircrew experienced G-LOC : 144 (34.69%) |
| 3. | Aircrew with single G-LOC episode: 98 |
| 4. | Aircrew with two G-LOC episode: 35 |
| 5. | Aircrew with three G-LOC episode: 08 |
| 6. | Aircrew with four G-LOC episode: 02 |
| 7. | Aircrew with five G-LOC episode: 01 |
| 8. | Total G-LOC incidents: 205 |
| A. Based on rate of onset: |
| • GOR: 24 |
| • ROR: 96 |
| • SACM: 24 |
| B. Based on psycho-physiological symptoms: |
| • Type-I: 96 |
| • Type - II: 48 |
| Type of run | Number | Incapacitation period | ||
|---|---|---|---|---|
| Abs | Rel | Total | ||
| GOR | 24 96 24 | 12.09±4.5 | ||
| ROR | 10.31+4.16 | |||
| SACM | 10.95±2.90 9.17±4.06 |
|||
| 6.88±3.67 | ||||
| 7.79±4.33 21.26+6.31 |
||||
| 17.20+5.75 | ||||
| 18.73±4.90 | ||||
| Total | 144 | |||
| PeakG | 7G | 8G | 9G | Others |
| No. | Incapacitation period: | Total | ||
|---|---|---|---|---|
| Abs | Rel | |||
| Type -1 | 96 | 10.88+4.05 | 7.63±3.98 | 18.40+5.71 |
| Type - II | 48 | 11+4.76 | 8.75±3.75 | 19.75+6.07 |
| Number | 15 | 37 | 44 | Nil |
| Parameter | Study-I | Study-II | Present Study-A | Present Study-B |
|---|---|---|---|---|
| Period of study | 91-94 | 91-97 | 91-2001 | Jan98-Mar2001 |
| No. of subjects | 134 | 259 | 415 | 154 |
| Relaxed GOR-tol | 4.97 ±1.03 | 4.89±0.75 | 5.01G±0.77 | 5.24 ±0.85 |
| Straining GOR-tol | 7.77±0.92 | 8.0+0.10 | 7.9G+0.96 | 7.92+0.98 |
| 9 Gz during GOR | - | 7.7% | 12.5% | 17.35% |
| Relaxed ROR-tol | 4.17±0.79 | 4.3 ±0.45 | 4.27G±0.47 | 4.29 ±0.51 |
| Straining 7Gz ROR | 98.51% | 99.61% | 98.8% | - |
| Straining 8Gz ROR | 92.54% | 93.4% | 97.13% | 97.4% |
| Straining 9Gz ROR | 70.15% | 78% | 90.45% | 92.2% |
| Average SACM-tol | 165.7sec | 180sec | 179.2sec | 178.45sec |
| G-Loc incidence | 35.8% | 35.5% | . 34.69% | 33.77% |
| Course duration | 6days | 12days | 12 days | 12 days |
| Type of run | Number of G-LOC | Absolute | Incapacitation period Relative |
Total |
|---|---|---|---|---|
| GOR | 04 | 10.25 ±3.86 | 14.00±i.63 | 24.25 ±3.5 |
| ROR | 37 | 10.64+4.69 | 8.75±3.92 | 19.40±6.72 |
| SACM | 11 | 11.00+3.76 | 12.00+4.24 | 23.00±5.04 |
| Total | 52 |
| No. Trained | No. of G-LOC | Percentage of G-LOC | |
|---|---|---|---|
| Total no. of pilots | 154 | 52 | 33.77 |
| Pilots done Stage-IIA | 30 | 06 | 20 |
| Pilots not done Stage-IIA | 124 | 46 | 37 |
Discussion
It is seen from Table 5 above that relaxed ROR tolerance and average duration of SACM tolerance is significantly higher in our pilot population. All other parameters are significantly higher in US Air Force population. This difference can be explained by virtue of ethnic differences and differences in centrifuge capability. The USAFSAM has a centrifuge, which is capable of onset rate of 6 G/sec and offset rate of 3 G/sec with seat tilt back facility. The seat tilt back itself increases G-tolerance by 0.5 G or more in relaxed subjects [1, 11]. In contrast, our centrifuge has onset and offset rates of 1 G/sec and we have not used any seat tilt back facility. The incidence of G-LOC is lower and recovery from GLOC faster if the rates of onset/offset are higher [13]. In certain cases G-LOC occurs at the offset at the lower level particularly when pilot is exhausted from a high-G run because of slower rate of offset. Such cases can be prevented if the offset rates are higher. The chance of G-LOC is higher in GOR runs [9] but in our centrifuge most cases occurred during ROR runs and this can be attributed to the slower onset and offset rates. Table 7 shows that less number of pilots has suffered from psycho physiological symptoms during G-LOC. It is seen from Table 8 that the period of incapacitation varies with the type of run and is longer during GOR runs than in ROR or SACM runs. Table 9 shows that more number of G-LOC cases have occurred with higher levels of G-values during ROR runs. Table 10 shows that time of recovery is prolonged in G-LOC episodes associated with myoclonic jerks than without them.
Comparison of results of previous two studies in IAM with the present Study-A is shown in Table 9. The results show minor changes in most of the parameters. Significant changes have been seen in incidence of G-LOC cases. Decreased incidence of G-LOC in both the later studies may be attributed to introduction of Stage-IIA course, which has reduced the total percentage of G-LOC cases in the present study (Table 13). The combined result of ten years (Study-A) with the last three years results (Study-B) shows significant increase in GOR (relaxed) tolerance and straining 9 G ROR tolerances in the later study. These can be attributed to complete digitization since 1998 and better instrumentation leading to increase in pilot motivation. At the end of the course, the pilots fill a questionnaire to opine on the usefulness of the course. More than 50% of pilots found it very useful and rest found it useful whereas very few gave equivocal/negative response. Most of them wanted this course to be repeated after an interval of 2-5 years.
Review of world literature indicates that inspite of high incidence of G-LOC; centrifuge training is useful and safe. Retrospective analysis by Whinnery [14] of 500 cases of G-LOC episode in human centrifuge showed no long-term squeal. Whinnery and Jones [15] have reported cases of recurrent G-LOC episodes [3, 4, and 5] within 6-15 minutes in four subjects without any squeal. In all our studies [2, 3, 4] no untoward incidences associated with G-LOC have been reported so far. In IAF, a subject is monitored by continuous ECG monitoring throughout the run under the supervision of a medical officer, which is not done routinely in many air forces including USAF [1]. Deliberate induction of G-LOC to reduce incapacitation time in subsequent G-LOC has been recommended by certain workers in the field [16]. However, it is unethical and not recommended in IAM training. Inadvertent G-LOC during centrifuge training is unavoidable but safe.
As regards the usefulness of the course is concerned earlier studies have shown in-flight incidence of G-LOC as 10.8% in IAF pilots [3]. But, the actual incidence may be double as half the pilots are not able to recollect the incident. So, actual incidence may be 22%. Brazilian and US Air Force estimate a rate of 21% and 24% respectively [4]. The aircrews were asked to fill a questionnaire after six months of flying following the course. A total of 64 pilots have returned the questionnaire till date. Out of this one pilot has reported an incident of G-LOC after the course and he could recover consciousness in time and ejected safely. This was reported in a study in 1997 [4]. The above feedback also shows 75% of pilots consider the course useful. Very few gave equivocal or negative response. 50% of pilots wanted this course to be repeated after a certain interval. 73% acknowledged the need for this kind of course =in modern combat environment. These facts further emphasize the utility of the course and it is self-explanatory. In USAF, after introduction of high G course, the accident rate due to G-LOC fell from 4 per million flying hours (pmfh) to 1.3 accidents pmfh [9]. The course may be made safer and productive if better centrifuges with higher capabilities of onset and offset rates are used. It will definitely reduce the incidence of GLOC during centrifuge training and allow better monitoring of pilots with more physiological parameters.
Conclusion
G-LOC episodes are unavoidable during centrifuge training. A modern centrifuge with higher onset and offset rates with active control by the pilot will probably reduce the incidence of G-LOC during centrifuge training. Centrifuge should have acceleration capabilities matching that of modern aircrafts for ideal transfer of training. This will make the training more effective and realistic and also increase the research potential. All those who have undergone centrifuge training have received it with enthusiasm. Our experience has shown that centrifuge training has a high acceptability with the pilot population and it has helped in teaching the correct practice of AGSM, thereby increasing their G-tolerance. Thus, it has contributed to flight safety by reducing the risk of G-LOC, thereby preventing aircraft accidents.
References
- Centrifuge training of fighter aircrew. The Indian experience. Ind J Aerospace Med. 1994;38(2):84-8.
- [Google Scholar]
- G-induced loss of consciousness (G-LOC) in the Indian Air Force. Ind J Aerospace Med. 1992;36(1):1-5.
- [Google Scholar]
- Prevention of loss of consciousness with positive pressure breathing and supinating seat. Aviat Space Environ Med. 1988;59:20-22.
- [Google Scholar]
- G-tolerance enhancement: straining ability comparison of aircrew men non-aircrew men and trained centrifuge subjects. Aviat Space Environ Med. 1982;53:232-234.
- [Google Scholar]
- Human tolerance to high sustained +Gz acceleration. Aviat Space Environ Med. 1972;43(7):708-712.
- [Google Scholar]
- +Gz-induced loss of consciousness accidents USAF experience 1982-1990. Aviat Space Environ Med. 1992;63(1):60-66.
- [Google Scholar]
- The use of a fixed base simulator as a training device for high sustained or ACM (air combat manoeuvring) +Gz stress. Advisory Group for Aerospace Research and Development. In: North Atlantic Treaty Organization; AGARD-CP-189. 1976. p. :A8-1-6.
- [Google Scholar]
- Centrifuge training of USAF fighter pilots (Abstract) Aviat Space Environ Med. 1984;55:467.
- [Google Scholar]
- Standardization Agreement (STANAG) No. 3287 AMD, Minimum requirements for selection training and employment of aircrew in high sustained Gz environment. Military agency for standardization, North Atlantic Treaty Organization.
- [Google Scholar]
- The effect of Gz offset rate on recovery from acceleration induced loss of consciousness. Aviat Space Environ Med. 1990;61(10):929-34.
- [Google Scholar]
- Recognising Gz induced loss of consciousness and subject recovery from unconsciousness on a human centrifuge. Aviat Space Environ Med. 1990;61(10):406-11.
- [Google Scholar]
- Recurrent Gz induced loss of consciousness. Aviat Space Environ Med. 1987;58(10):943-7.
- [Google Scholar]
- Gz induced loss of consciousness: a case for training exposure to unconsciousness. Aviat Space Environ Med. 1987;58(5):468-72.
- [Google Scholar]




