Translate this page into:
Analysis of Initial Medical Flight Screening of Aircrew Candidates: USAF vis-à-vis IAF
Abstract
Air Forces worldwide have specified comprehensive medical standards for aircrew selection for flying duty. The medical morbidity pattern is expected to be different between aircrew candidates and trained aviators. There has been no published study in the USAF which analyzes medically disqualifying conditions among aircrew applicants for flying duty. The present study was thus carried out to analyze the physically disqualifying, waiverable and permanently disqualifying conditions during initial flight screening of USAF aircrew candidates. Relevant data was collected from the medical database maintained at Aeromedical Consultation Services (ACS), USAF School of Aerospace Medicine. The disabilities pattern was compared with that of trained aircrew and published data of IAF. During the period of the study, a total of839 aircrew applicants underwent initial medical evaluation for flying duty at ACS. 374 candidates (44.5%) were made physically disqualified due to various medical conditions. Waiver was granted in 310 cases (36.9%) and 64 candidates (7.6%) were permanently disqualified from flying duty. Among the permanently disqualified candidates, ophthalmological conditions (65 %) were found to be the most common cause followed by systemic medical conditions (27%). Color vision defect was noted to be the most common ophthalmic condition resulting in permanent disqualification. The medical disabilities amounting to rejection in aircrew candidates were much different to those of trained aircrew. Comparison with similar data revealed significant differences in morbidity patterns among aircrew candidates with of IAF.
Keywords
Medical standards
physically disqualifying
waiverable and permanently disqualifying

Introduction
High standards of physical fitness is desired among aircrew candidates to meet the increasing demands of military aviation environment. Stringent medical standards have been established in many Air Forces world wide for selection of the fittest candidate not only for effective completion of flying training, but also for further employability as a military aviator. In order to meet this objective, USAF has stipulated comprehensive medical standards for flying duty in AF1 148-123 [1]. This document specifies requirements, medical standards, recording and procedures for medical examination for flying duty. Medical conditions are considered physically disqualifying for aviation duty, if they do not fulfill the requirements of medical standards. However, depending upon the seriousness of the condition, a waiver may be granted on case to case basis as per the specifications laid down in USAF waiver guide [2].
Physically disqualifying conditions which are not able to meet the waiver consideration would result in permanent disqualification and rejection of candidates for flying duty.
The rate of permanent flying disqualifications among trained aviators has been reported to be 0.18% to 4.1% per year in two different USAF studies [3,4]. A study on waivers for disqualifying medical conditions in US Naval aviation personnel mentions a waiver recommendation of 68% among designated aviation personnel [5]. Similar reviews of permanent grounding has been published by Canadian and Russian Air Forces [6,7]. The most common physically disqualifying conditions have been reported to be coronary artery disease, hypertension, degenerative spine disease and back pain, diabetes mellitus, migraine headache, asthma and drug/alcohol abuse.
Literature search revealed only a few of the published studies on the medical causes of disqualifications among aircrew candidates. Analysis of initial medical examination of aircrew applicants in Indian Air Force has shown that a significant number of candidates (36.2%) were rejected for flying duty [8]. Similarly, for women cadets the rate of rejection has been reported to be as high as 55% [9]. In USAF, there has been no published study analyzing initial medical flight screening among aircrew applicants. The pattern of medical morbidities prevalent in aircrew applicants would be different than those of trained aircrew because of the significant age difference. Further, there is a likelihood that the causes of medical rejection for flying duty during entry would significantly differ in different Air Forces. This is not only because of the racial and ethnic variance in population but also due to the major differences in the laid down medical standards. In view of this, the present study was carried out to analyze the physically disqualifying, waiverable and permanently disqualifying conditions during initial flight screening of USAF aircrew candidates and to compare these data with that of Indian Air Force.
Material and Methods
Medical database maintained at Aeromedical Consultation Services (ACS), USAF School of Aerospace Medicine, Brooks City Base was utilized for collection of data. The medical records of US AF applicants for flying duty for one year period were reviewed to find out physically disqualifying, waiverable and permanently disqualifying conditions for flying duty. For this study physically disqualifying conditions were defined as those medical conditions which do not fulfill the requirements of medical standards. Waiverable conditions were those physically disqualifying conditions where waiver was granted. Those disqualifying conditions where waiver was not granted were the permanently disqualifying conditions and are the causes of rejection for flying duty. Some candidates have multiple disabilities, however the condition most likely resulting in permanent disqualification was defined as the cause of rejection. A comparative analysis was done with similar data from Indian Air Force to understand the basis of medical rejection during initial flight screening. Comparisons were also made with published data on medical disabilities amounting to rejection from aircrew duty in trained USAF aircrew.
Results and Analysis
During the period of the study, a total of 839 aircrew applicants underwent initial medical evaluation for flying duty. 374 candidates (44.5%) were made physically disqualified due to various medical conditions. Aeromedical waiver was granted in 310 cases (36.9%) and 64 candidates (7.6%) were permanently disqualified from flying duty. Physically disqualifying and permanently disqualifying conditions are depicted in Fig -1 and Fig - 2 respectively.

- Physically disqualifying conditions (n=374)

- Permanently disqualified conditions (n=64)
A comparative analysis of physically disqualifying conditions which were granted waiver and those which were permanently disqualified is shown in figure - 3.

- Comparative analysis of physically disqualifying conditions
Ophthalmological conditions (57%), systemic medical conditions (25%) and otolaryngological conditions (13%) were found to be the major physically disqualifying conditions. However, the major causes of permanent disqualification were the ophthalmological (65%) and systemic medical conditions (27%). The remaining 8% of the disabilities leading to rejection was constituted by radiological spinal abnormality (3%), surgical (3%) and otolaryngological conditions (2%).
Among ophthalmological conditions, refractive errors constituted the most common physically disqualifying condition, however waiver was granted in many cases (Fig - 4). Common ophthalmological conditions responsible for permanent disqualification were defective colour vision (40%), refractive errors (19%), inadequate depth perception (12%) and keratoconus (12%) (Ref Fig - 5).
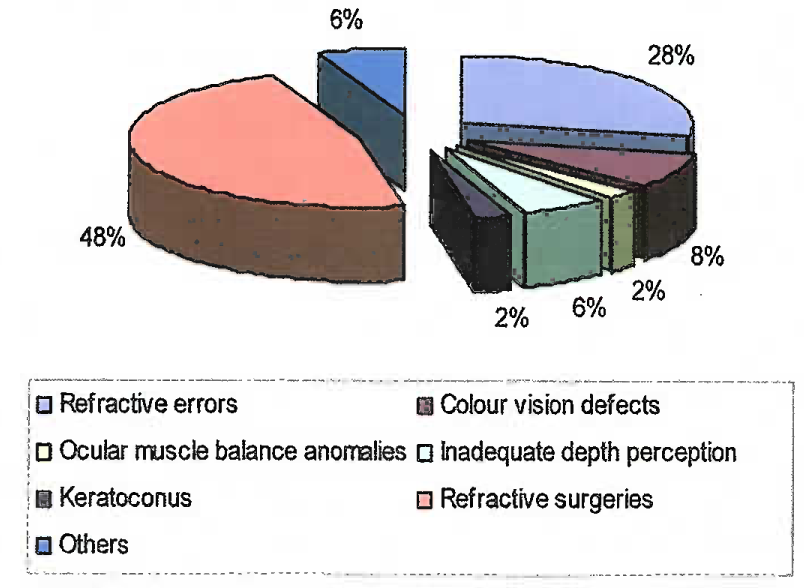
- Physically disqualifying ophthalmological conditions (n=169)

- Permanently disqualifying ophthalmological conditions (n=42)
Systemic medical disabilities were the next common disqualifying conditions in this population (Ref Fig - 6 and 7). Neurological abnormalities (42%) constituted the most common condition, but waiver was granted in 87% of cases.
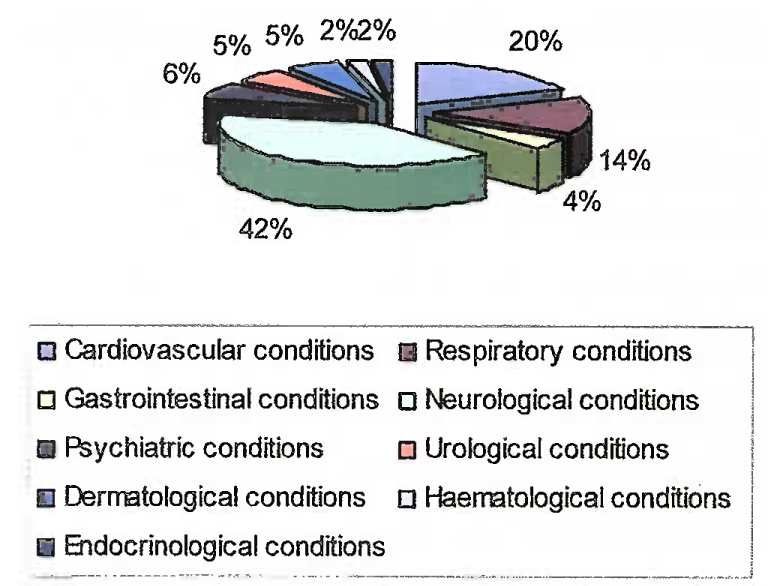
- Physically disqualifying systemic medical

- Permanently disqualifying systemic medical conditions (n=17)
Out of 49 disqualifying otolaryngological conditions, waiver was granted in 48 cases. The only case which was permanently disqualified was due to substandard hearing. Only 3 cases of radiological spinal abnormality were recorded, out of which one candidate who had scoliosis of more than 20° (Cobb’s method) was rejected. Surgical conditions were detected in 5 cases, and 2 of them were permanently disqualified. All the disqualifying cases of anthropometric incompatibility (7 cases) and orthopedic conditions (5 cases) were granted waiver.
Discussion
Initial medical flight screening is intended to select the fit individuals who would be able to meet the operational requirement in aviation environment. To meet this objective, the aircrew candidates should fulfill the qualifying medical standards. In the present study, the prevalence of physically disqualifying conditions was 44.5%, which is similar to most of the Air Forces. However, provision of the waiver recommendations for conditions which are considered not to interfere with flying duty has reduced the overall permanent disqualification rate to as low as 7.6% as compared to that of Indian Air Force (36.2%) and Royal Jordanian Air Force (31.3%) [8, 10].
| Permanently disqualifying conditions | USAF | IAF [8] |
|---|---|---|
| Ophthalmological conditions | 65% | 37% |
| Systemic medical conditions | 27% | 7% |
| Otolaryngological conditions | 2% | 9% |
| Radiological spinal abnormality | 3% | 24% |
| Anthropometric incompatibility | 0% | 14% |
| Surgical conditions | 3% | 3% |
Ophthalmological conditions constituted the most common disqualifying disabilities in both the Air Forces which shows the high visual standards laid down for flying duty. Colour vision defect was the most common ophthalmic condition (40%) accounting for disqualification in USAF, in contrast to refractory errors (76%) in Indian Air Force. This can be explained on the basis of very stringent established colour vision standard and use of highly sensitive color vision testing modalities in the USAF. There were 99 cases of corrective refractive surgery, out of which only one case who also presented with corneal haze was rejected and rest all were given waiver. This is in contrast to IAF study which reported rejection of two cases with history of corrective refractive surgery.
Radiological abnormalities have been reported to be responsible for 24% of disqualification in the IAF and 20% in Royal Netherlands Air Forces [8, 11]. In contrast, this represented only 3% in USAF. This can be explained on the basis of differences in medical screening standards in different Air Forces. The USAF offers medical waiver for most of the asymptomatic radiological abnormalities.
The anthropometric incompatibility has been reported to be one of the leading causes of disqualification in the IAF [8]. However, in the present study none of the USAF candidates were disqualified on this account. The IAF has most of its trainer and fighter jet aircraft produced in other countries, which are not designed for Indian population and thus it is no surprise to expect anthropometric incompatibility among IAF aircrew candidates. On the other hand most of the military aircraft in USAF have been indigenously designed to meet the anthropometric requirements of its population.
Comparative analysis of permanently disqualifying conditions between aircrew applicants and trained aircrew is depicted in Fig - 8. The most prevalent disqualifying.
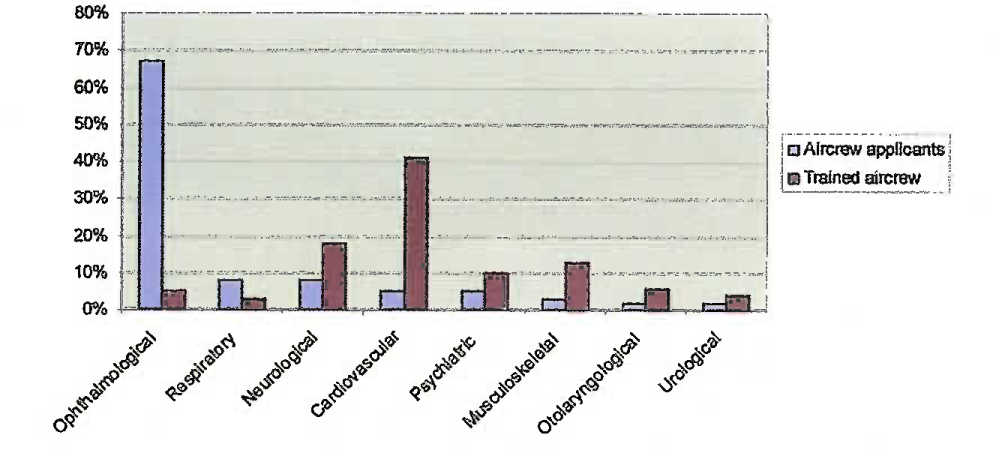
- Comparative analysis of permanently disqualifying conditions:
Aircrew applicants vis-à-vis trained aircrewconditions among trained aircrew have been reported to be cardiovascular (41%), neurological (18%) and musculoskeletal conditions (13%). The ophthalmological conditions accounted for only 5% of disqualification [3]. This is quite different than those in applicants. This can be related to wide variances in the age and the laid down medical standards between the two groups.
Conclusion
This study provides a broad overview of the medical disabilities resulting in disqualification for flying duty among USAF aircrew applicants. It also highlights the differences in permanent disqualifying conditions with that of trained aircrew and compares the similar data from Indian Air Force. Even though the prevalence of physically disqualifying conditions during initial entry was found to be quite high, the numbers of candidates permanently disqualified were very few. Ophthalmological conditions in general and colour vision defects in specific remained the most common cause of rejection.
References
- U.S. Air Force Instruction 48-123. In: Medical examinations and standards. Washington, DC: U.S. Air Force Headquarters; 2001.
- [Google Scholar]
- USAF Waiver Guide San Antonio, Tx: U.S. Air Force School of Aerospace Medicine. In: Brooks City Base. 2009.
- [Google Scholar]
- Permanent flying disqualifications of USAF pilots and navigators (1995-1999) Aviat Space Environ Med. 2002;73:1117-21.
- [Google Scholar]
- Medical disqualification in USAF pilots and navigators. Aviat Space Environ Med. 1984;55:332-6.
- [Google Scholar]
- Waivers for disqualifying medical conditions in U.S. Naval aviation personnel. Aviat Space Environ Med. 1995;66:401-7.
- [Google Scholar]
- Permanent grounding and flying restrictions in Canadian Forces pilots: a 10 year review. Aviat Space Environ Med. 1991;62:513-6.
- [Google Scholar]
- Number of chronic conditions and professional longevity of aviators. Aviat Space Environ Med. 1997;68:373-7.
- [Google Scholar]
- Retrospective analysis of initial medical examination of aircrew applicants in the Indian Air Force. Ind J Aerospace Med. 2006;50:44-9.
- [Google Scholar]
- An analysis of initial medical examination of women cadets in the Indian Air Forces. Ind J Aerospace Med. 2006;50:50-3.
- [Google Scholar]
- Medical causes of dismissal in candidates selection for pilots in Royal Jordanian Air Force. Aviat Space Environ Med. 2005;76(3(Section 1)):204.
- [Google Scholar]
- Degenerative changes of the spine of fighter pilots of the Royal Netherlands Air Forces (RNLAF) Aviat Space Environ Med. 1999;70(11):1057-63.
- [Google Scholar]




