Translate this page into:
Aeromedical Concerns and Lessons Learnt during Oxygen Jump at Dolma Sampa
Abstract
Background:
Combat Free Fall (CFF) is practiced during peace time for operational readiness of the air warriors during war. Free fall is practiced at different altitudes and the operations are named accordingly i.e. Static line, High Altitude Low Opening (HALO) and High Altitude High Opening (HAHO). Since it is difficult for the radar to detect accurately a military aircraft beyond 20,000 feet AMSL (Above Mean Sea Level), troops can fall from its belly silently, undetected. Even though CFF operations materialized during the times of Cold War, Vietnam War and also in Operation Iraqi Freedom, there is a scarcity of literature evidence regarding paratroopers and their physiological effects when exposed to aviation stressors in such missions.
Operation:
A CFF with Oxygen (also referred to as Oxygen jump) was performed by nine parajumpers over Dolma Sampa. The event was unique in its kind as it was a high altitude parajumping (>20,000 ft AMSL) with supplemental oxygen and the Drop Zone (DZ) was also at a high altitude i.e. 14,090 ft AMSL. Under such circumstances, it becomes important to consider the various aeromedical stressors like hypoxia, hypobaria, hypothermia, decompression sickness (DCS), acute mountain sickness (AMS), etc. that played a part during such jumps and thereafter during the landings at the DZ. The paper discusses these aeromedical concerns involved in preparation prior to the mission and combating the various aeromedical stressors during the Oxygen jump and after landing at DZ.
Keywords
Combat Free Fall
Hypoxia
Hypothermia
Decompresion sickness
High altitude parajump

INTRODUCTION
Combat Free Fall (CFF) is an important war strategy. It is a mean to penetrate into enemy areas, without crossing the border on ground and also for fast deployment of troops at the exact location of attack in the enemy territory. The operations have the advantage of time, location, precision and element of surprise for the enemy [1]. It is practiced regularly as the peace time training for achieving appropriate level of skill and competency. The operation is undertaken at different altitudes and the operations are named accordingly i.e Static line, High Altitude Low Opening (HALO) and High Altitude High Opening (HAHO).
During the Cold War in 1950s, US Army and Marine Corps were deploying paratroopers as secret missions [1]. The technique of Combat Free Fall was also used for combat during the Vietnam War and during Operation Iraqi Freedom [2]. The strategic advantage provided by such operations was that, it was difficult for the radar to detect a military aircraft and the free falling troops from it. However, such high altitude para-dropping operations are associated with life threatening aeromedical stressors in the form of hypoxia, decompression sickness (DCS), hypothermia, etc. In addition, the possibilies of non-deployment of parachute, landing injuries, apprehension of being fired at or captured in the enemy territory also exist.
A Combat Free Fall with Oxygen (also referred to as Oxygen jump) was performed over Dolma Sampa, Sikkim from a military transport aircraft from an altitude of 20,000 ft and 23,000 ft. The Drop Zone (DZ) at Dolma Sampa was located at 14,090 ft AMSL. The 25 member team had 11 parajumpers, 03 Dispatchers & 01 Master Dispatcher along with 04 Aircrew, 01 Aviation Medicine Specialist, 04 Observers and one 01 photographer. A search and rescue (SAR) team was also positioned at the DZ. The 11 member SAR team which embarked the military helicopter had 05 Aircrew (Pilot, Co-pilots, Flt Gun, Flt Eng), 03 Para Jump Instructor (PJI), and 03 Supporting crew (01 Med officer, 01 Met Asst & 01 Ops Asst). This paper discusses the aeromedical concerns and lessons learnt during the course of these Oxygen jumps.
Summary of Events
A day prior to the flight, the paratroopers were briefed regarding the aeromedical stressors of the high altitude (20,000 and 23,000 ft) jumps i.e. hypoxia, hypobaria, hypothermia and DCS. A detailed clinical history was taken to ensure that none of the para troopers had any illness including common cold, throat pain, cough, tiredness or fatigue. In addition, all of them underwent a complete ENT examination. They were advised to refrain from alcohol consumption 24 hrs prior to the sortie and were also briefed about the use of oxygen especially during Pre-breathing.
On D day, all 25 members were given Pre-breathing of oxygen for duration of 30 min through the oxygen console of the aircraft. In addition, the dispatchers were on portable oxygen and were moving around to supervise the paratroopers and their equipments. The inflight SpO2 was monitored using a digital pulse oximeter.
Once the aircraft climbed to 20,000 ft and over the DZ, cabin decompression was initiated by opening the ramp door. Meanwhile, two of the paratroopers were declared unfit for the jump by the dispatchers due to technical complications related to para trooping. They were advised to take off their parachutes and continue breathing 100% Oxygen from the Oxygen console.
The remaining nine paratroopers got ready for the jump. Eight of them jumped from an altitude of 20,000 ft. Following this, the aircraft ascended to an altitude of 23,000 ft. The mission coordinator performed the Oxygen jump from 23,000 ft. Then the ramp door was closed and cabin was repressurized. 100% Oxygen inhalation was continued till the appropriate cabin pressurization was achieved.
During this process, two dispatchers complained of uneasiness. The pulse oximeter readings revealed that SpO2 had fallen below 60%. They were made to sit comfortably, hold their mask properly with both hands and breathe 100% Oxygen. After a while both of them felt better with increase in SpO2, which reached a value well above 90%. Their symptoms were resolved completely by the time the aircraft landed at its pre-designated location.
All the parajumpers landed safely at the DZ where they were received by the ground support team. The duration of stay at DZ was 45 min. Thereafter, the paratroopers and other crew were brought back to the unit by helicopter. A detailed clinical history for occurrence of any joint pain, ear pain or sinus pain was sought. They were also examined for any sinus tenderness and haemorrhage or oedema in tympanic membrane. There was no significant ENT or other clinical findings in any of the paratroopers. The other members in the aircraft also had no clinical symptoms or signs.
DISCUSSION
The Parajumps carried out over Dolma Sampa were HALO type. The operation was unique because the jumps were attempted at high altitude (>20,000 ft AMSL) and drops were made on a Drop Zone which was also located at a high altitude i.e. 14,090 ft AMSL. Being a drop at High Altitude Area (HAA), there was a need to address the issues like hypoxia, hypobaria, hypothermia, DCS along with Acute Mountain Sickness. It is not only the paratroopers who were at risk of getting affected by the aeromedical stressors, the crew of aircraft that took part in the mission were also at a similar risk.
The removal of nitrogen that is normally dissolved in the tissues and body fluids was accomplished by breathing 100% Oxygen before exposure to reduced pressure. This procedure is termed as ‘pre-oxygenation’ or ‘denitrogenation’. Though, DCS is theoretically possible during any flying mission undertaken above 18,000 ft AMSL, it is not a major threat below 22,000 ft AMSL [3]. Altitude chamber studies have revealed that at 22,500 ft and 25,000 ft, pre-breathing Oxygen for one hour is highly beneficial in reducing the incidence of DCS, as compared to no pre-breathing of oxygen. It also delays the onset of DCS, the incidence being less than 6% during the first 90 min of exposure. [4]. For high altitude parajumping (>20,000 ft AMSL), it is essential to carry out a pre-breathing with 100% Oxygen for 30-45 min prior to depressurisation (or opening up of the ramp) of the cabin, to minimize the risk of DCS. This pre-breathing requirement is over and above a personal bail out system that is mandatory for the jump [5]. In USAF, the de-nitrogenation schedules for HALO missions involves 30 minutes of pre-breathing with 100% Oxygen for exposures between 18,000 and 25,000 ft [6]. In our case also, 30 min pre-breathing was performed on board the aircraft through the Oxygen console, prior to opening of the ramp. Once depressurization was achieved and the ramp was opened, the jump was performed while breathing oxygen through personal oxygen system.
Breathing air above 20,000 ft could expose the crew to Critical Hypoxia, where the physiological compensatory mechanisms may not be able to maintain the homeostasis against the hypoxic insult. There could be rapid deterioration of mental and cognitive performance, and even risk of unconsciousness with little or no warning [7]. This further strengthens the importance of pre-breathing and use of supplemental oxygen during jump. However, symptoms of hypoxia can be experienced if there is an improper fitment of the Oronasal mask or any fault in the onboard oxygen system. This could have been the possible cause of hypoxia in case of the two despatchers. Though they were on 100% Oxygen throughout, they did not notice that their mask had become loose while they were preparing the paratroopers for the jump. Once they sat down holding their mask with both hands and continued breathing 100% oxygen, their symptoms got resolved. Therefore, monitoring of SpO2 throughout the mission was an important lesson in this operation.
Hypothermia is another factor that needs to be considered while carrying out an Oxygen jump at or above 20,000 feet AMSL. Considering the fact that there is drop of mean temperature at a lapse rate of -1.98°C per 1000 feet from mean sea level to 36,089 feet [8], the ambient temperature at 20,000 ft would be 39.6°C less than that of MSL and at 23,000 ft would be 45.5°C less than that of MSL. During takeoff the environmental temperature at the parent airfield was recorded to be 18°C. Hence, the ambient temperature at 20,000 ft and 23,000 ft could be calculated as approximately -22°C and -28°C respectively. Moreover, the DZ being situated at an altitude of 14,090 feet AMSL, the ambient temperature could be calculated as approximately -10°C. Under such circumstances, appropriate protective measures against cold injuries must be considered both for the paratroopers and the ground rescue team positioned at DZ. Also, extra caution needs to be exercised while measuring SpO2 after opening the ramp door of the aircraft. Exposure to sub zero temperature (after removal of gloves to measure SpO2) might cause hypothermia induced vasoconstriction in the digits and also could be a reason for spurious readings in the finger pulse oximetry.
Since the window period available to the paratroopers for making the jump is small, the success of such a mission requires proper coordination and in-flight communication. When the ramp door was opened at 20,000 ft AMSL, the ambient noise made it difficult to converse in spite of the availability of a two-way communication. Therefore, the paratroopers were instructed to use either the sign language (to raise their right hand if experiencing uneasiness) or to write their problem on the paper provided. This is where the importance of Effective Performance Time (EPT) and Time of Useful Consciousness (TUC) come into play.
The Time of Useful Consciousness (TUC) at 22,000 feet AMSL is 5-10 min [9]. But for the paratroopers, TUC would be approx. 30-50% below that of a rested person owing to their heightened anxiety and physical activities involved prior to the jump. A probable TUC among the paratroopers is shown in Fig. 1, and it depicts the TUC at 20,000 ft and 23,000 ft to be approx 8 min and 4 min respectively [5]. This needs to be taken into account while determining the window period for jump from the aircraft.
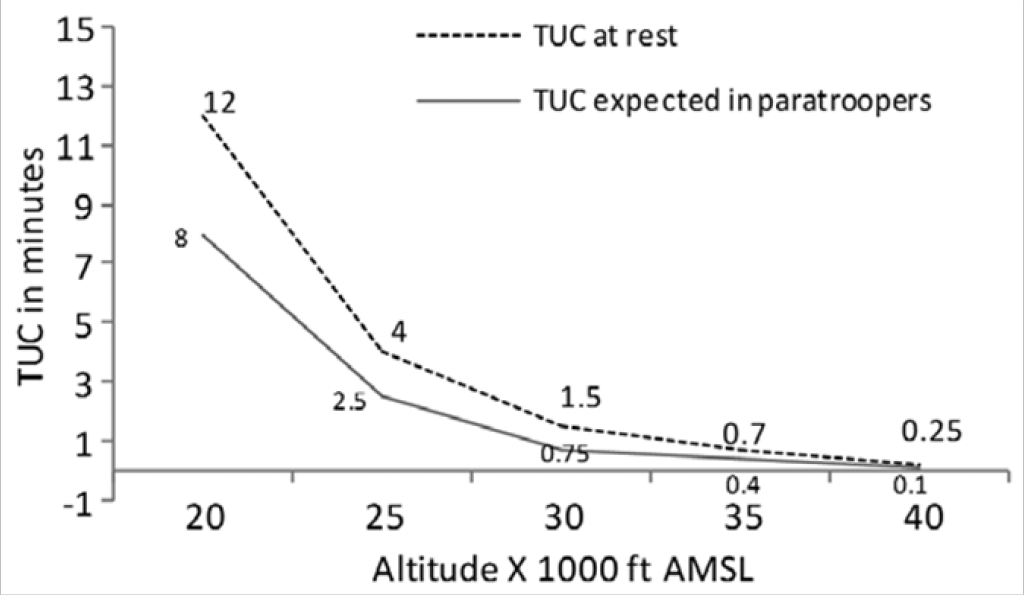
- Mean TUC at rest vs TUC expected in paratroopers
The duration of stay at the drop zone (located at a high altitude i.e. 14,090 ft AMSL) was 45 minutes. Though a stay at high altitude for such a small duration of time does not require prior acclimatization, the same would be required during actual combat situations. Under such circumstances, the role of acclimatization and use of Acetazolamide tablets for prevention of Acute Mountain Sickness becomes important [10].
LESSONS LEARNT AND RECOMMENDATIONS
Hypoxia is a real possibility in all high altitude jumps and could affect the paratroopers if appropriate measures are not followed. It is known that early recognition of symptoms and prompt intervention could prevent serious complications. Therefore, hypoxia indoctrination training of paratroopers and dispatchers could be a value addition to their existing training curriculum.
In absence of such training, appropriate Audio-Visual aids on various aeromedical stressors related to high altitude i.e. hypoxia, hypobaria, hypothermia, DCS, Acute Mountain Sickness, etc. could be incorporated during mission briefing prior to high altitude jumps.
The importance of correct fitment of mask to prevent inboard leak especially for the dispatchers who is to breathe from a portable oxygen system was another lesson learnt. This could be ensured by the Aviation Medicine Specialist/ Medical Officer who is a part of the medical team.
None of the paratroopers had any incidence of otitic barotrauma during the mission. This confirms their ability to equalize the middle ear pressure with the ambient pressure change during rapid free fall. Valsalva maneuver, which is an established procedure to equalize middle ear pressure, cannot be performed by the paratroopers with oxygen mask. It is therefore important to train them for adopting the passive methods like swallowing, moving the jaw, yawning, etc.
CONCLUSION
The era of CFF has arrived and it is going to stay, as more and more such operations are bound to take place in future warfare, due to the strategic advantages provided by such missions as well as the element of surprise for the enemy. The successful execution of any CFF mission depends on the ability of the air warriors to combat the various aeromedical stressors as discussed in the paper. Though very few scientific studies have been undertaken regarding the physiological effects of such aeromedical stressors on a paratrooper, it is imperative to incorporate the knowledge available and lessons learnt during the course of every CFF practiced during peace time for operational readiness of the combatants during war.
References
- Decompression chamber runs for screening and training of HALO paratroopers and training of fighter aircrew. Ind J Aerospace Med. 2008;52(2):35-43.
- [Google Scholar]
- Falling into history: ODA 074 makes first combat halo jump into Iraq In: Special Warfare. Vol 21. US Army John F. Kennedy Special Warfare Center and School; 2008. p. :15-18.
- [Google Scholar]
- Oxygen systems, pressure cabin and clothing In: Gradwell DP, Rainford DJ, eds. Ernsting’s Aviation and Space Medicine (5th ed). Florida (USA): CRC Press; 2016. p. :112-29.
- [Google Scholar]
- Altitude decompression sickness between 6858 and 9144m following a 1h prebreathe. Aviat Space Environ Med. 2005;76:34-38.
- [Google Scholar]
- Supplemental oxygen for paratroopers and sky divers. Defence Science Journal. 2012;62(1):51-57.
- [Google Scholar]
- Decompression Sickness During C-130 High Altitude Operations In: The Proceedings Of The 1990 Hypobaric Decompression Sickness Workshop Edited by Andrew A. Pilmanis. AL-SR-1992-0005. p. :424.
- [Google Scholar]
- Hypoxia and hyperventilation In: Gradwell DP, Rainford DJ, eds. Ernsting’s Aviation and Space Medicine (5th ed). Florida (USA): CRC Press; 2016. p. :49-64.
- [Google Scholar]
- The Earth’s atmosphere In: Gradwell DP, Rainford DJ, eds. Ernsting’s Aviation and Space Medicine (5th ed). Florida (USA): CRC Press; 2016. p. :3-12.
- [Google Scholar]
- Mechanisms of action of acetazolamide in the prophylaxis and treatment of acute mountain sickness. J Appl Physiol. 2007;102(4):1313-22.
- [Google Scholar]




