Translate this page into:
A Retrospective Analysis of Low Backache with Associated Lumbo-Sacral Disabilities in Military Aviators
Abstract
Introduction:
Back pain is a common complaint amongst aircrew of all aircraft irrespective of stream. Cases of Low Backache (LBA) with radiological and structural abnormalities that were evaluated at the Department of Human Engineering (HE), Institute of Aerospace Medicine (IAM), Indian Air Force (IAF) have been analyzed for various causes over a period of 3 years from June 2012 to July 2013.
Methods:
Cases reporting with LBA during the period from June 2012 to July 2015 have been chosen as sample for the study (n-99). The distribution of LBA across the various aircraft streams, the cause for LBA, precipitating factors, treatment undertaken and period of unfitness for flying has been analysed.
Results:
Out of all the cases (n=406) reporting to Department of HE at IAM for evaluation of Musculoskeletal disabilities during this three year period, a total of 99 cases amounting to 24%, were cases of LBA with structural or radiological abnormalities. Amongst the three streams, incidence of Low backache was highest in the fighter stream (43%) followed by helicopter stream (34%) and transport stream (23%). The commonest aetiology for the LBA is attributed to Disc Degenerative Disease of Lumbo-Sacral Spine (53%) and the number of such cases across various streams was comparable. Spinal fractures were highest in Fighters (11%) and lowest in Transports (1%). 55% of the LBA cases had insidious onset without precipitating factors. Majority of the cases underwent conservative treatment (91%) and only 9% cases underwent surgical intervention. The period of medical unfitness for flying varied from less than 12 weeks to more than 200 weeks. The majority of the aircrew (78%) were upgraded to unrestricted flying medical category within 200 weeks. Some of the cases (18%) had not reached clinical finality during the period of the study.
Conclusion:
Lumbo-Sacral spinal disabilities are a common morbidity in military aviators. Twenty four percent of all musculoskeletal disabilities were cases of LBA with radiological or structural abnormalities. Certain radiological findings are associated with specific streams such as the association of spinal fractures with Fighter and Helicopter aircrew. Whereas, the incidence of disc degenerative disease is similar across the streams. 55% of the backache cases gave no history of any precipitating factors. Number of cases of Mechanical LBA was similar in fighter and helicopter aircrew and least in transport aircrew. 73% of the cases could be re-flighted within the permissible period of observation on ground and amongst these re-flighted aircrew, the majority of cases (90%) underwent only conservative treatment. The role of focused physiotherapy and rehabilitation program on the prognosis of LBA needs to be deliberated as the same has not been analysed in this study.
Keywords
Military aviators
Lumbo-Sacral spine
Re-flighting
Aeromedical

Introduction
Lumbo-sacral (LS) spine disabilities are a cause of concern in aircrew as they can critically affect their flying duties. All candidates as well as serving personnel aspiring for flying duties are thoroughly screened for spinal abnormalities at the time of induction into flying branch. However, there are a large number of military aviators who develop low backache (LBA) owing to LS spinal conditions. Low back pain or Low backache is a poorly defined term but represents the symptom of pain or discomfort felt in the back or buttocks [1]. Back pain is a common complaint amongst aviators of various aircraft streams [2].
All LBA cases are evaluated at the Institute of Aerospace Medicine (IAM), the aviators with LBA, after being evaluated by the concerned clinical specialists, undergo functional evaluation by Aerospace Medicine specialists at the Department of Human Engineering (HE) for their aeromedical disposition [3]. Disposal of LBA cases are determined by the likelihood of the condition getting aggravated in the aviation environment owing to the nature of flying duties expected of that individual and also its influence on the aerospace safety.
Records of all cases with musculoskeletal abnormalities were scrutinized and out of these records, the cases of LBA with radiological or structural abnormalities were further analysed for various factors such as stream wise distribution of LBA, the aetiologies, probable precipitating factors, modality of treatment undertaken and period of observation on ground.
Material & Methods
All Low Backache cases associated with radiological and structural LS disabilities that were evaluated at the Dept of HE over a period of three year (June 2012 to July 2015) were taken as the sample for the study. These records maintained at the Dept of HE, IAM were scrutinized and the relevant information required for this study was extracted. The data for this study comprises of military aircrew diagnosed as cases of ‘Low Backache’ with radiological/ structural findings severe enough to have placed them in a non-flying medical category.
The data was analysed based on the following:-
Number of aircrew reporting for evaluation of LBA with radiological/ other structural abnormalities.
Stream-wise distribution of aircrew suffering from LBA.
LBA with respect to their aetiology.
Stream wise distribution of leading causes of LB
Precipitating factors for LBA.
Period of observation in non-flying medical category.
Modality of treatment in these cases.
Results
A total of 406 serving aircrew comprising of 166 from the fighter stream, 122 from the transport stream and 118 from the helicopter stream were evaluated at the Dept of HE at IAM for various musculoskeletal conditions. The distribution of musculoskeletal disabilities which had reported between the periods of June 2012 to July 2013 is shown in Fig-1. Out of these 406 cases, 99 aircrew (n=99) presented with LBA (24%), which were associated with radiological / structural findings and was the sample for this study.
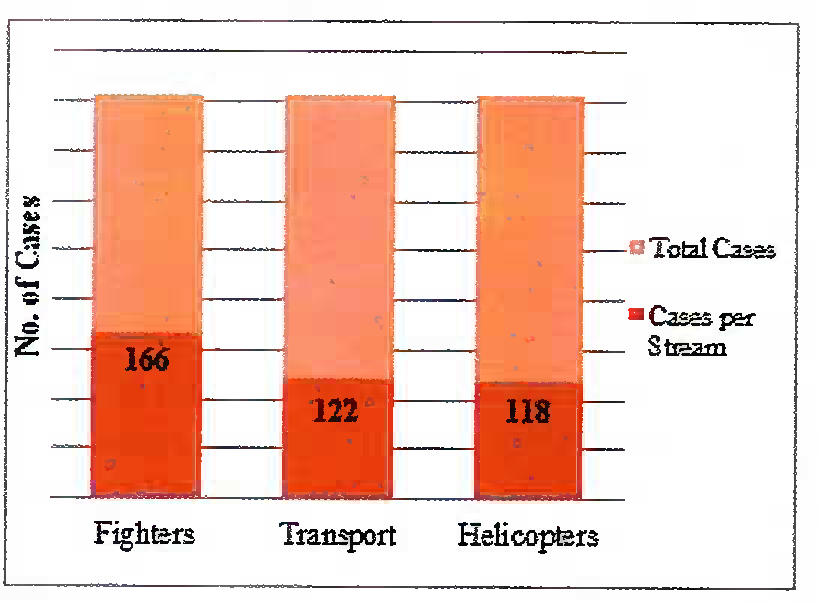
- Streamwise Distribution of Musculoskeletal Disabilities (N = 406)
Amongst the three streams, the number of LBA cases were highest in Fighter (F) aircrew (43%), followed by Helicopter (H) aircrew (34%) and Transport (T) aircrew (23%) which is represented in Fig-2.
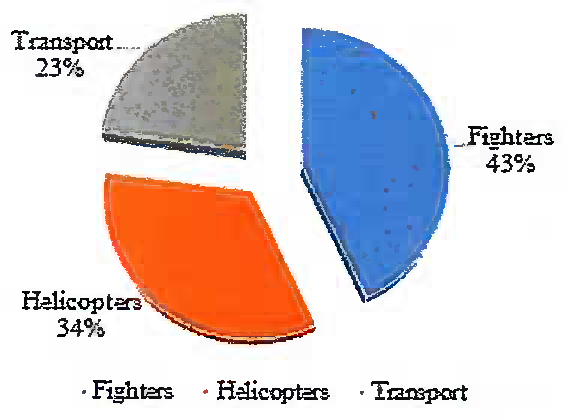
- Distribution of LBA
These LBA cases (n=99) were further studied for specific diagnoses. The disabilities comprised of Disc Degenerative diseases including Prolapsed Intervertebral Disc (PIVD), Fracture of Vertebrae (LS Segment), Spondylosis, Spondylolysis, Spondylolisthesis, Schmorl’s nodes, Nerve root compression, Facet joint arthropathy, Sacroilitis and Caries spine. These disabilities were grouped into specific diagnoses and their incidence was analysed. The bulk of the disabilities were due to Disc degenerative disease (53%), followed by Inflammatory 17%, Mechanical LBA (13%), Fracture (8%), Anatomical (5%) and others (4%). The distribution of disabilities are represented in Fig-3.
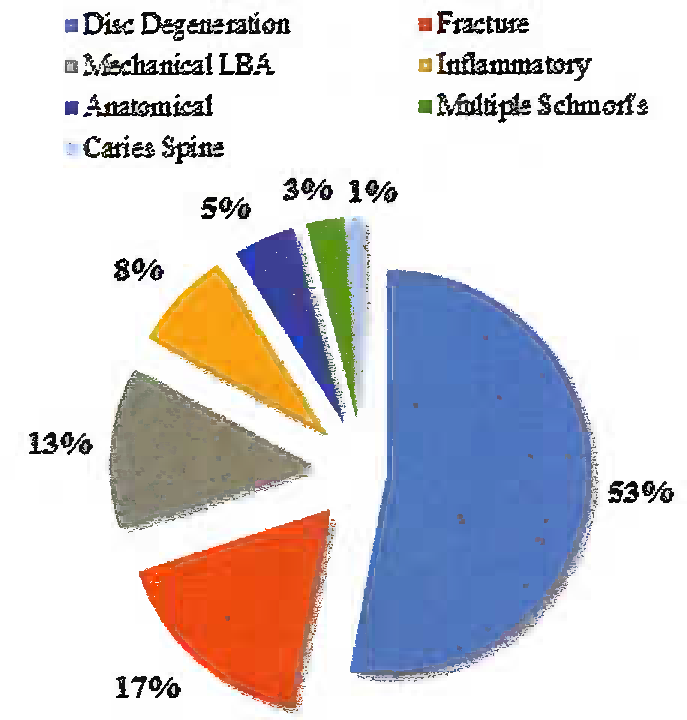
- Diagnosis for LBA
Amongst the leading causes for LBA that emerged from the study, there is a variation in the distribution of these disabilities across various aircraft streams. Incidence of Disc Degenerative Disease and inflammatory causes are similar across all the aircraft streams as shown in Fig-3, whereas there is a considerable difference in the distribution of Vertebral Fractures involving LS Spine. Of the total No of cases of Vertebral fracture involving LS spine, 64.71% (n=ll) of the cases were seen in fighter aircrew and the distribution of the same being 29.41% (n=5) and 5.88% (n=l) in Helicopters and transport aircrew respectively. Mechanical LBA was seen to be of equal distribution in Fighters (46.15%) and Helicopters (46.15%) and least in transport aircrew (7.69%). The distribution of disabilities is represented in Fig-4.
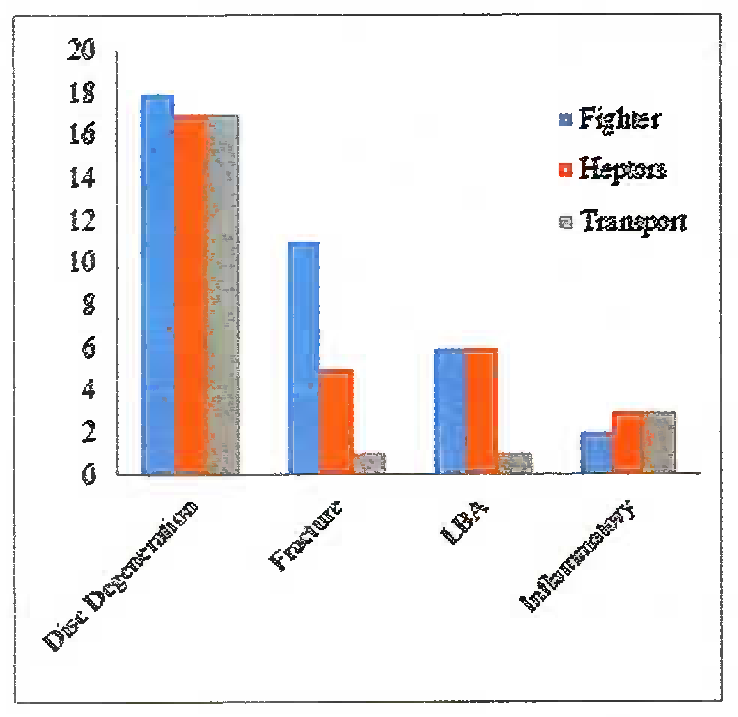
- Disability Vs Stream
Analysis of the probable precipitating factors associated with the various causes of LBA in the aviators revealed that the majority of cases (55%) did not give any history of likely precipitating cause for their backache. Such cases were grouped as ‘insidious’ LBA cases. The other probable precipitatingfactors are; Post ejection injuries (13%), Hard/crash landing (11%), accidents, other than aircraft accidents (10%), Games and sports (10%) and miscellaneous (1%). The various precipitating factors causing LBA are shown in Fig-5.
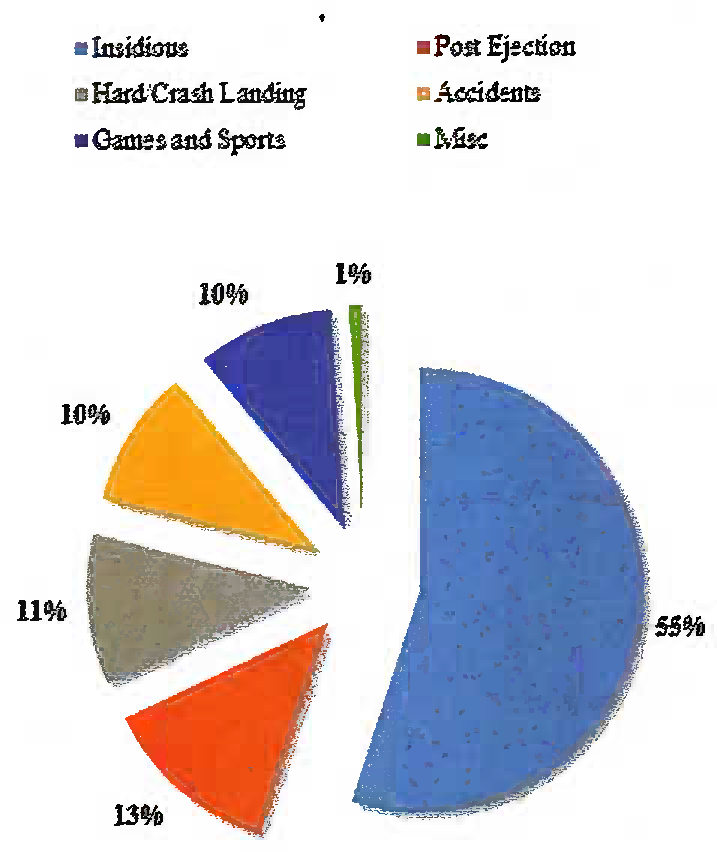
- Probable Precipitating Factors
The data available at the Dept of HE from June 2012 to July 2015 was analysed to establish the period of unfitness for flying. The data collated was grouped into various blocks of weeks viz. upto 12 wks, 13-24 wks, 25-48 wks, 49-96 wks, 97-200 wks and more than 200 wks. In addition cases were also grouped as ‘Pending’ cases and ‘Permanently Unfit for Flying’ cases. 78% of the cases achieved flying medical category within 200 weeks. 18% of the cases were still in nonflying medical category as these cases had not reached clinical finality and required further observation ‘on ground’. One of these 18% cases had exceeded the maximum period of observation ‘on ground’ after which the aviator has to be declared permanently unfit for aircrew duties [3]. The various periods of observation of the sample during the study period are shown in Fig- 6 & 7.
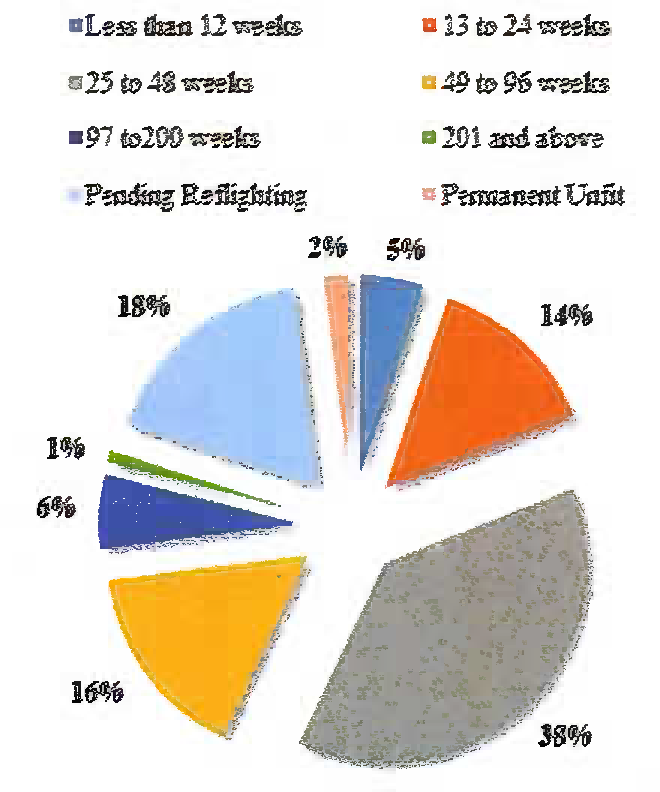
- Observation Period
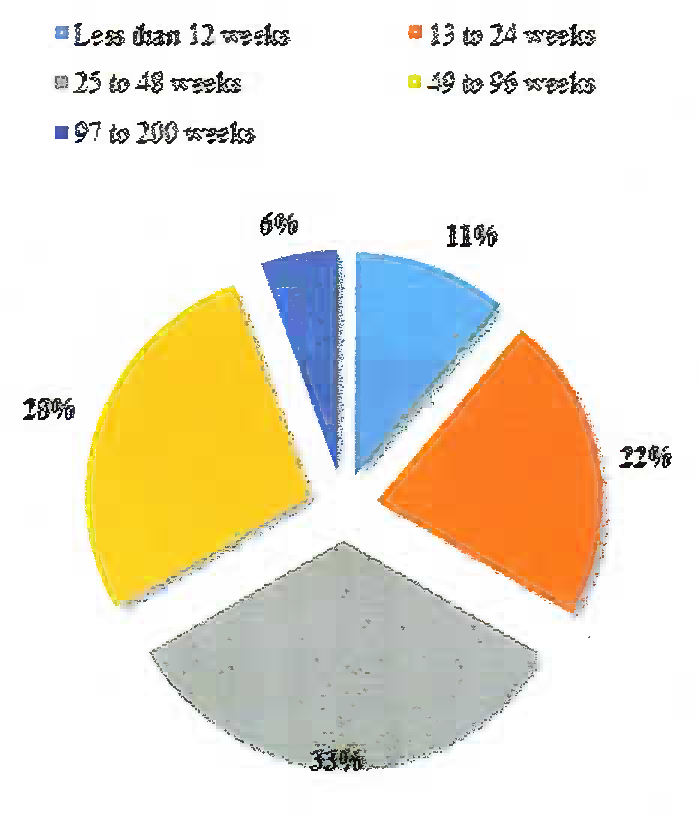
- Observation Period : Pending Cases
Amongst the 18 aircrew who were in temporary non-flying medical category, 11% had been under observation for less than 12 wks, 22 % for 13-24 wks, 33% for 25-48 wks, 28% for 49-96 wks and 6% for 96-200 weeks.
The treatment modality undertaken for the management of all LBA cases was analysed. The majority of cases (91%) underwent conservative treatment and only 9% of all the cases underwent surgical intervention (Fig-8).
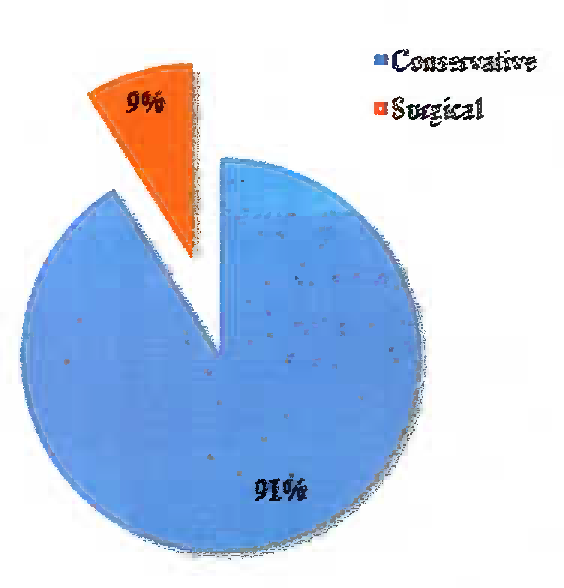
- Treatment Modality
On analysis of the re-flighted cases, it was observed that 90% of them were managed conservatively while only 10% underwent surgical treatment. Even amongst the pending cases, 95% were undergoing conservative management and only 5% had undergone surgical treatment. In respect of the permanently unfit cases, both the cases had undergone conservative management only. The breakup of the treatment undergone by the cases is shown in Fig-9.
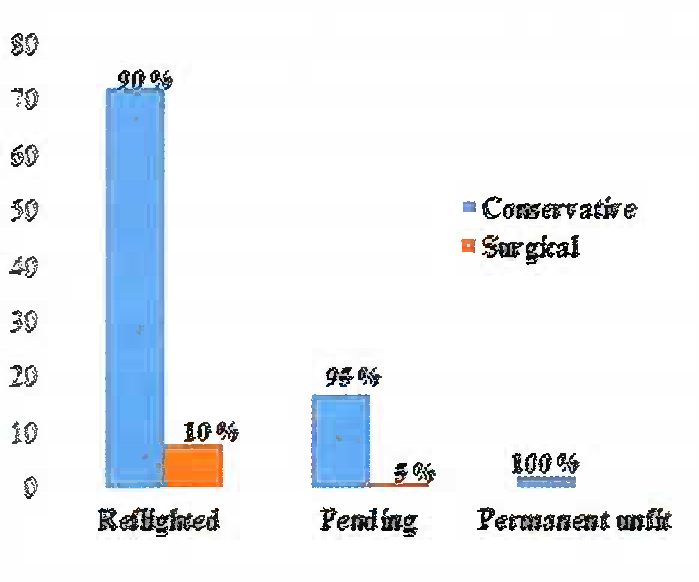
- Treatment vs Disposal
Discussion
LBA is a common complaint amongst military aviators [2,4]. LBA in aviators can arise from a number of lumbosacral disabilities viz. injuries resulting from ejection, crash/ hard landing, games and sports, repeated loading of the spine etc [5,6]. Interestingly, the majority of aviators presenting with Low Back Pain did not give history of any precipitating factor. Rather, the majority of the backache reported by our aviators were insidious in onset.
In this study, the maximum number of aircrew with backache were from fighter stream. Taneja et al studied the IAF aircrew reporting to IAM with musculoskeletal disabilities in the period 2001-2003. Of the total number of aircrew evaluated (n=232), 48.2% (n=212) were cases of musculoskeletal abnormalities involving the spine. Amongst the Fighter, Transport and Helicopter streams the maximum musculoskeletal disabilities were reported by aircrew from the fighter stream (53.4%) [5]. In aviation, LBA has critical significance due to the possibility of aggravationof pain during flight, owing to exposure to aviation stressors such as high G forces, vibration, bad posture, ejection forces and impact forces encountered during hard landings [6,7]. When the various causes for backache were considered, it was observed that Disc Degenerative Disease was associated with the majority of aviators complaining of LBA [5]. Disc Degenerative Disease arising out of aviation stressors are not specific to a single stream, the number of cases of LBA with Disc Degenerative Disease was (52%) which was the highest for a particular condition. LBA precipitated by fractures was highest in Fighters (13%), because of the increased prevalence of hard landings and ejection injuries compared to the other stream. The inflammatory conditions leading to backache was similar across the three streams.
Incidence of Mechanical Backache was higher in fighter and helicopter pilots as compared to transport pilots probably because of high G loads and vibration respectively [6,7]. Mechanical back pain is the general term that refers to any type of back pain caused by placing abnormal stress and strain on muscles of the vertebral column [8]. Typically, mechanical pain results from bad habits, such as poor posture, poorly- designed seating and incorrect bending and lifting motions. Patients generally present with a history of an inciting event that produced immediate low back pain. The most commonly reported histories include the following:
Lifting and/or twisting while holding a heavy object
Operating a machine that vibrates
Prolonged sitting
Involvement in a motor vehicle collision
Falls
Studies have shown the benefits of focused rehabilitation in early recovery of back disabilities [9]. In this study also, it was observed that most of the cases (91 %) underwent conservative management and various periods of observation on ground prior to upgradation to flying category. At present, IAM is the only center undertaking evaluation and aeromedical disposition of any aircrew with musculoskeletal disabilities. On the other hand, the treatment and rehabilitation of such cases are followed-up in their dependent Hospitals, Station Medicare Centres and/or Medical Inspection rooms. This study has not analysed the role of focused physiotherapy or rehabilitative programs in the early re-flighting of the aviators as the same is currently not imparted at IAM.
57% of the LBA cases were re-flighted within 48 weeks and 73% within 96 weeks. As per the Indian Air Force Publication (IAP) 4303, cases requiring observation in temporary non-flying medical category are to be certified permanently unfit for flying at the end of two years [3]. Only one case was under observation for a period of over 200 weeks. This aircrew was not awarded a permanent non-flying medical category as he was detected to have another disability (unrelated to LBA) for which he had to be observed ‘on ground’ hence he was allowed to continue in temporary non-flying medical category under ‘waiver’ from the competent authority.
In this study the psychological aspects of LBA have not figured as all cases analysed had an organic cause for the back pain. Psychological overlay associated with the backache, if any, has not been documented in any of these cases.
Conclusion
This study provides an insight into LBA in aircrew which is associated with radiological or structural abnormalities. Certain radiological findings are associated with specific streams such as the association of spinal fractures with Fighter and Helicopter aircrew. On the other hand, the incidence of disc degenerative disease was found to be similar across the streams. Majority of the backache cases (55%) did not give history of any precipitating cause for their backache. Number of cases of Mechanical LBA was the equal in aircrew from the transport and helicopters and least amongst the transport aircrew. A large majority of the cases (73%) could be re-flighted within the permissible period of observation on ground and 90% of these cases could be upgraded to a flying category with conservative management alone. Therefore, rehabilitative programs with focused physiotherapy play a meaningful role in recovery of aviators with LBA. The study of this aspect is likely to be beneficial.
Disclaimer
The opinions expressed in this article are those of the author & do not reflect the official views of the Indian Air Force or the Indian Society of Aerospace Medicine
References
- Low backache: Synopsis of causation Nottingham: Ministry of Defence Publication; 2008.
- [Google Scholar]
- Back symptoms in aviators flying different aircraft. Aviat Space Environ Med. 2012;83:702-5.
- [Google Scholar]
- A Retrospective Analysis of Musculoskeletal Disabilities in Military and Civil Aircrew. IJASM. 2008;52(1):8-13.
- [Google Scholar]
- Diagnostic categories among 232 military aircrew with musculoskeletal disabilities. Aviat Space Environ Med. 2005;76:581-5.
- [Google Scholar]
- Low backache in fighter pilots. Indian Journal of Aerospace Medicine. 2000;44(2):1-6.
- [Google Scholar]
- Radiological review of spinal injuries sustained during combat flying, hard landing and ejection 96-98. Indian Journal of Aerospace Medicine. l994;43(1):29-34.
- [Google Scholar]
- Mechanical Low Back Pain Everett C Hills MD, MS; Stephen Kishner, MD, MHA. 2015. Assessed from https//www.emedicine.medscape.com/article/310353-ovcrvicwon01Aug2015
- [Google Scholar]
- Psychological factors affecting recovery in aircrew with musculoskeletal disabilities. IAM Departmental Project No IAM/195/20.
- [Google Scholar]




