Translate this page into:
Maintenance of Mental Alertness During Total Sleep Deprivation of Short Duration: A Double Blind, Placebo Controlled, Comparative Study Between Modafinil 100 mg and 200 mg
Abstract
Introduction:
Short duration sleep deprivation is a more practical eventuality in military air operations. Efficacy of oral administration of single dose of 100 and 200 mg Modafinil, on maintenance of mental alertness following 18-h of continuous wakefulness extending to 24-h was examined.
Methods:
In a double blind, crossover, placebo-controlled, repeated measure design, seven healthy male participants (with each 'case' serving as his own 'control'), were assessed for their mental alertness and subjective perception of sleepiness and fatigue in an extended period of wakefulness of 24 hours. In addition, feedback was obtained on known untoward effects of Modafinil through a questionnaire.
Results:
A significant main effect of sleep deprivation was observed on mean reciprocal reaction time with a significant interaction effect between the two main effects (sleep deprivation x drug intervention). There was a significant increase in the number of lapses with sleep deprivation, which was not found significant with administration of Modafinil. These effects were more observable with 200 mg Modafinil than 100 mg. Subjective perception of sleepiness and fatigue were significantly increased with Placebo and 100 mg Modafinil, which was not found significant with 200 mg Modafinil. The occurrence of untoward effects with Modafinil was no more than that with Placebo.
Discussion:
Several researchers have expressed the requirement of exploring the possibility that a lower dose of Modafinil, which will be relatively free from side effects, may also be effective in the maintenance of performance. Whereas, this may be true for long duration sleep deprivation requiring multiple doses of drug intervention, for mission demanding forced wakefulness of 24 h, single dose of 200 mg Modafinil appears to be a better option.
Conclusion:
Administration of Modafinil in a dosage of 200 mg is more effective than 100 mg in maintaining mental alertness and improving subjective sleepiness and fatigue during short duration total sleep deprivation.
Keywords
Modafinil
Sleep Deprivation
Mental Alertness
Fatigue

Learning Objectives:
Even short duration of acute sleep deprivation can have a significant degradation of mental alertness.
During short duration total sleep deprivation that permits administration of a single dose of medication, Modafinil in a dosage of 200 mg is more effective than 100 mg in maintaining mental alertness and improving subjective sleepiness and fatigue.
Introduction
Modern air operations are characterized by the need to maintain persistently high levels of performance, even in the presence of Total Sleep Deprivation (TSD). The negative effects of sleep deprivation cause decrement in performance reducing margin of safety with vulnerability to accidents and errors [1]. In the aviation scenario, it may lead to aviation errors and accidents [2].
Under conditions of extended wakefulness and sleep deprivation, pharmaceutical intervention offers an effective short term solution to maintain mental alertness and cognitive performance. Among the most common pharmacological agents which have been experimented in this regard are Amphetamine and Modafinil. Modafinil [(±)-2-(benzhydrylsulfinyl) acetamide] [3] an 'analeptic' agent, which also has 'eugregoric' properties, is known to have beneficial effects on measures of alertness and cognitive performance during sleep deprivation [4]. Modafinil is also claimed to produce less cardiovascular stimulation than amphetamine [5], another psychostimulant in use, and has minimal effects on sleep architecture [6]. Because of its wakening properties, low toxicity and near absence of tolerance producing effects, Modafinil has been referred to as a 'molecule of military interest'.
The efficacy of repeated doses of 200 mg of Modafinil in maintenance of performance has been shown up to 44 – 48 hours of continuous wakefulness [7,8]. Caldwell et al [9] found that 200 mg of Modafinil every 4 hour maintained the simulator flight performance of pilots at near-well-rested levels despite 40 hour of continuous wakefulness, but that there were complaints of nausea and vertigo (likely due to the high dosage used). Similar beneficial effects were seen on measures flight performance up to 37 hour period of continuous wakefulness with 100 mg doses of Modafinil (administered every 5h) in a more recent study with U.S. Air Force F-117 pilots [10,11]. The lower dose produced these positive effects without causing the side effects noted in the earlier study.
The previous studies, however, have involved very long duration of sleep deprivation. Short duration, rather than long duration acute sleep deprivation is a more practical eventuality in military air operations. Further, such a period of sleep deprivation would permit single dose of drug administration potentially eliminating possible side effects of the drug. Exploration of optimal doses of Modafinil during such a period of sleep deprivation has substantial practical relevance to military aerospace operations. Examination of the efficacy of 100 and 200 mg oral administration of Modafinil, on maintenance of mental alertness following 18 hours of continuous wakefulness extending to 24 hours, among Indian male volunteers, was the desired exploration of the present study.
Materials and Methods
In double blind, crossover, placebo controlled, repeated measure design, seven healthy male participants (with each 'case' serving as his own 'control'), were examined for their mental alertness and subjective perception of sleepiness and fatigue in an extended period of wakefulness of 24 hours. Mental alertness was objectively assessed by Psychomotor Vigilance Task (PVT) monitor. Subjective appreciation of sleepiness was assessed by Stanford Sleepiness Scale (SSS) and fatigue by Chalder Fatigue Questionnaire (CFQ). In addition, feedback was obtained on known untoward effects of administration of Modafinil through a questionnaire. The study involved longitudinal evaluation of mental alertness in each participant assessed on three different sessions, one with Placebo (P), one with Modafinil 100 mg (M1) and one with Modafinil 200 mg (M2), taken after ~18 hours of continuous wakefulness and then extended to 24 hours of continuous wakefulness. A gap of minimum one week was maintained between the sessions.
All the participants were briefed on the first day of the study regarding its protocol and significance. An informed written consent was obtained. They avoided any alcoholic beverages and had a restful sleep the night before the commencement of the study. On the day of experiment, they reported at 0745h after having breakfast. The 'wake time' was recorded that varied from 0550 - 0615h. The first evaluation was made at 0800h. Thereafter, they remained awake, returned to their normal place of work and did only routine works throughout the day not involving strenuous activities, did not have any alcoholic beverages and reported at 2130h after dinner. Following this, they were not permitted to have tea or coffee throughout the period of assessment. The second evaluation was made at 0000h (Mid Night), which corresponded to ~ 18 hours of continuous wakefulness. Following this, drug intervention was done; the participant received either Placebo, or Modafinil 100 mg, or Modafinil 200 mg. The drugs or placebos were administered in capsules with identical appearance. Thereafter, periodical evaluations were made every hour for next 6 hours till 24 hours of continuous wakefulness. Participants were permitted to talk to each other or read newspapers/magazines in between the evaluations. A block diagram of the protocol is given in Table -1:-
| Evaluation 1 | 0800h [Baseline] |
|
|||||
| Evaluation 2 | 0000h [~18 hours of continuous wakefulness] Placebo/ Modafinil 100 mg/Modafinil 200 mg |
||||||
| Evaluation 3 | 0100h |
|
|||||
| Evaluation 4 | 0200h | ||||||
| Evaluation 5 | 0300h | ||||||
| Evaluation 6 | 0400h | ||||||
| Evaluation 7 | 0500h | ||||||
| Evaluation 8 | 0600h [~ 24 hours of continuous wakefulness] |
||||||
The data were examined for normality of distribution using Shapiro Wilk's 'W' statistic to select an appropriate statistical test (parametric or non-parametric) for analysis. Repeated Measures (Analysis of Variance) ANOVA was used for analysis of PVT outcome measures. The two factors were pharmacological intervention (Placebo, Modafinil 100 mg or Modafinil 200 mg) and period of continuous wakefulness. For sleepiness/ alertness (SSS) and fatigue (CFQ) (measured on ordinal scales), appropriate non parametric tests (Friedman ANOVA) were employed. For occurrence of untoward effects with the administration of Modafinil 100 mg or Modafinil 200 mg, related sample Cochran's Q test was employed. Significance level was set as p<0.05. The level of significance is reported in the results.
Results
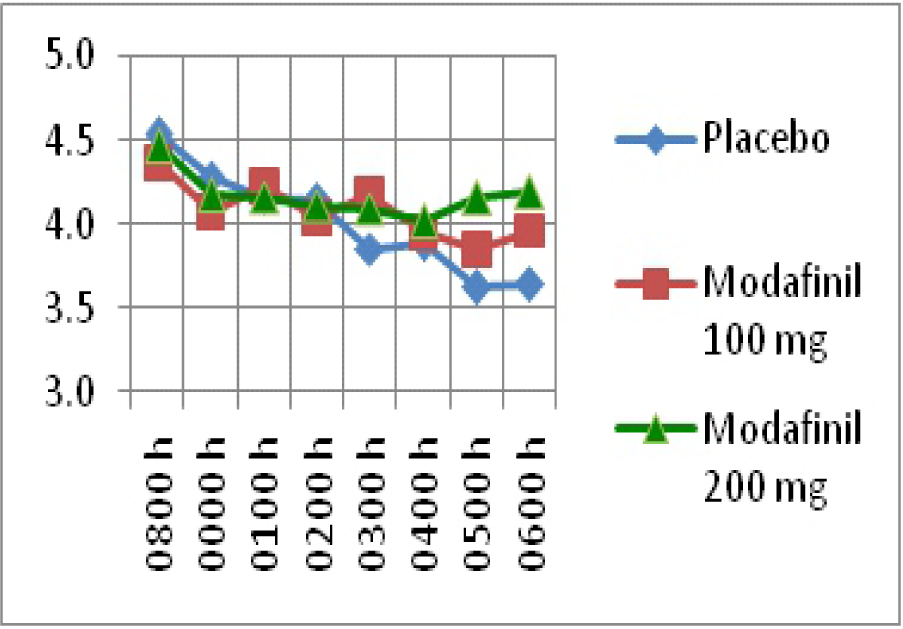
Analysis of PVT performance parameters revealed that there was a significant increase in number of lapses with continuous wakefulness in with Modafinil 100 mg (2= 11.43, p=0.12) and Modafinil 200 mg (2= 11.84, p=0.105). This is shown in Fig - 1. Mean Reciprocal Reaction Time (mean RRT) exhibited a significant main effect of sleep deprivation (F=5.142, p=0.0000) and interaction effect between the two main effects (sleep deprivation x drug intervention) (F=2.272, p = 0.011). This is shown in Fig - 2. It was also observed that administration of 200 mg of Modafinil was more effective than 100 mg of Modafinil, in maintaining mental alertness as assessed by their effects on primary PVT outcome measures (Fig - 1 & 2). The Mean Reaction Time (man RT) did not show any significant changes mental with sleep deprivation or drug intervention. alertness as assessed by their effects on primary PVT outcome measures (Fig - 1 & 2). The Mean Reaction Time (mean RT) did not show any significant changes 100 mg (2= 19.41, p=0.006).

- Lapses in PVT
- mean RRT (ms-1) in PVT
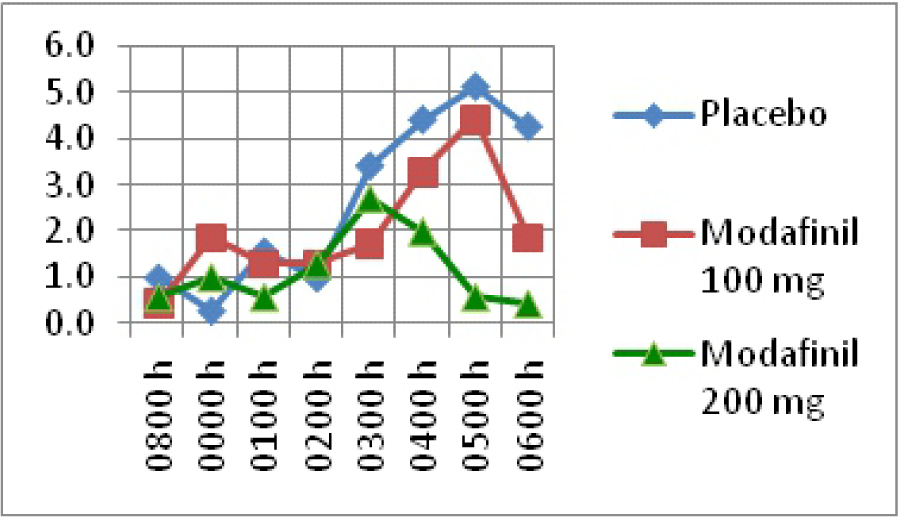
No significant effect with continuous wakefulness was observed with Modafinil 200 mg (2= 10.77, p=0.148). This is presented in Fig - 4. Related sample Cochran's Q test did not reveal any significant difference on the occurrence of untoward effects between Placebo, Modafinil 100 mg & Modafinil 200 mg at 0300 h and 0600 h.
- Subjective Sleepiness Score

- Subjective Fatigue Score
Discussion
Deficits in performance after long periods of sleep deprivation are well established. However, results of studies examining performance during short sleep deprivation are inconsistent [12, 13]. In view of the above, a short time frame of 6 hours specifically chosen in the present study. Such a was period of sleep deprivation has substantial practical relevance to military aerospace operations that require high level of mental alertness and cognitive performance.
In the present study, a significant main effect of sleep deprivation was observed on mean reciprocal RT with a significant interaction effect between the two main effects (sleep deprivation x drug intervention). This effect was more demonstrable with 200 mg of Modafinil than 100 mg (Fig - 1). Due to its superior statistical properties and robustness to extreme values, mean RRT has been identified to have peak sensitivity to sleep loss among PVT measures. Modafinil was also seen to exert a significant and demonstrable beneficial effect on performance lapses. There was a significant increase in the number of lapses with sleep deprivation. However, with administration of Modafinil, the number of lapses was not significantly different than the baseline values.
This effect was again more demonstrable with 200 mg of Modafinil than 100 mg (Fig - 2). In addition to mean reciprocal RT, lapses serve as an appropriate primary PVT outcome, because they (a) reflect state instability (b) have high ecological validity that relates to risk in attention-demanding, real-world tasks (e.g. driving); and (c) are the most common outcome metric in the peer-reviewed literature [15]. The effects of Modafinil on these primary PVT outcome measures were thus observed to be important findings in these studies.
Further, it was also observed that administration of 200 mg Modafinil significantly improved subjective sleepiness and fatigue as compared to 100 mg Modafinil and Placebo. This is a very important observation when viewed in the light of findings by Caldwell et al [11] that 100 mg Modafinil can be an effective countermeasure against detrimental effects of sleep deprivation. Whereas, the study by Caldwell et al involved 37 hours of continuous wakefulness, the present study focused extended wakefulness of 24 hours. The observation simply means that, during short duration sleep deprivation, even if, Modafinil in 100 mg can maintain the mental performance, administration of Modafinil in a dosage of 200 mg will improve subjective percept of sleepiness and fatigue and, therefore, should be resorted to. Further, the possibility of side effects as a result of higher doses of Modafinil due to repeated administration, as was observed by Caldwell et al [11] is remote; as short duration sleep deprivation would only permit administration of a single dose. Similar findings were observed in the present study. The side effects were mild and it was indistinguishable if the untoward effects were due to Modafinil or sleep deprivation as the occurrence was comparable statistically.
Conclusion
Several conclusions can be drawn from the results of the present study. Firstly, even short duration acute sleep deprivation can have a significant degradation of mental alertness. Secondly, administration of 200 mg of Modafinil is more effective in comparison with 100 mg of Modafinil in maintaining mental alertness as well as improving subjective sleepiness and fatigue. This inference merits special attention because several researchers have expressed the requirement of exploring the possibility that a lower dose of Modafinil, which will be relatively free from side effects, may also be effective in the maintenance of performance. Whereas, this may be true for long duration sleep deprivation requiring multiple doses of drug intervention, for mission demanding forced wakefulness of 24 hours, single dose of 200 mg of Modafinil administered at midnight appears to be a better option.
Disclaimer
The opinions expressed in this article are those of the author and do not reflect the official views of Indian Air Force or the Indian Society of Aerospace Medicine
References
- Sleep/ Wakefulness Management in Continuous/ Sustained Operations. RTO Lecture Series 223 RTO-EN-016 AC/323(HFM-064) TP/39 (North Atlantic Treaty Organisation).
- [Google Scholar]
- Naps and Modafinil as counter-measures for the effects of sleep deprivation on cognitive performance. Aviat Space Environ Med. 1999;70:493-498.
- [Google Scholar]
- Cognition enhancement by Modafinil: A meta-analysis. Aviat Space Environ Med. 2012;83:685-9.
- [Google Scholar]
- Physician's Desk Reference, Modafinil. Physician's Desk Reference. Montvale, NJ: Thomson PDR; :1193-6.
- [Google Scholar]
- Disrupted sleep-wake rhythm and performance: advantages of Modafinil. Mil Psychol. 1995;7:165-9.
- [Google Scholar]
- Maintaining alertness and performance during sleep deprivation: Modafinil versus Caffeine. Psychopharmacology (Berl). 2002;159:238-47.
- [Google Scholar]
- A double-blind, placebo-controlled investigation of the efficacy of Modafinil for sustaining alertness and performance of aviators: A helicopter simulator study. Psychopharmacology(Berl). 2000;150:272-82.
- [Google Scholar]
- Brooks City-Base, TX: U.S. Air Force Research Laboratory; 2004 Jan Report No. AFRL-HEBRTR-2004-0003.
- [Google Scholar]
- Modafinil's effects on simulator performance and mood in pilots during 37 h without sleep. Avi at Space Environ Med. 2004;75:777-84.
- [Google Scholar]
- The effects of sleep deprivation on divergent thinking and attention processes. J Sleep Res. 1992;1(4):223-30.
- [Google Scholar]
- Effects of one night of sleep deprivation on hormone profiles and performance efficiency. Mil Med. 2001;166(5):427-31.
- [Google Scholar]
- Psychomotor vigilance performance : Neurocognitive assay sensitive to sleep loss. Sleep deprivation: clinical issues, pharmacology and sleep loss effects 2005:39-70.
- [Google Scholar]
- Maximizing sensitivity of the psychomotor vigilance test (PVT) to sleep loss. Sleep. 2011;34(5):581-591.
- [Google Scholar]




