Translate this page into:
Civil aircraft disaster management on naval air station: Challenges and concerns
-
Received: ,
Accepted: ,
On 06 Jan 05, at 2224 hrs a Sahara CRJ passenger aircraft made its final approach at Dabolim airport, Goa. At touchdown the aircraft undercarriage broke and it slithered down the runway on its belly. The airport was facing its most feared emergency, a civil aircraft accident with passengers on board. Incidentally Dabolim airport is a Naval airport and it was left for the Navy to respond to this accident.
The Indian Navy has several of its air stations in cities and most permit civil aircraft operations. Large bodied aircraft operate from these air stations and therefore the eves present danger of a civil aircraft accident remains every airbase commanders greatest fear. This Sahara aircraft accident and the muted response of the state agencies necessitated a re-look at the existing Airport Emergency Plan (AEP), lacunae in the existing system and steps to be taken to formulate and implement a new AEP. This was especially important as the responsibility of disaster management is shared between several agencies namely Airport Authority of India (AAI), the Indian Navy and the state administration.
This paper describes the steps taken to implement an AEP for Dabolim airport with full participation of multiple agencies (Governmental, State and Private); challenges faced and concerns which need to be resolved.
Airport Emergency and Medical Plan
Airport Emergency Plan (AEP) of Civil Airports is primarily based on guidelines provided by ICAO [1]. In formulating the same for Naval Airfields or any other military airfield, it is necessary to refer to two other documents/agreements. These are the Airport Authority of India (AAI) Act of 1994 and Memorandum of Understanding (MOU) between the Airport Authority of India (AAI) and the military service. The AAI act of 1994 defines the status of the Civil terminal on a military airfield. Jurisdiction over the Civil terminal on a military airfield rests with the AAI. The MOU between the AAI and the military service defines areas in which the Navy would provide assistance to the AAI. Medical support is usually not included in the MOU. A review of literature regarding aircraft disaster management was also carried out [2-7]
Ideally, the AEP should be in consonance with the existing State Disaster Management Plan as the state authorities are the primary responders in the event of an aircraft disaster. However, Goa state disaster management plan is not specific as regards to aircraft disasters being more of a general guideline in the event of any disaster. Further, the existing State disaster, management plan had not been tested in the form of partial/full scale exercise. There was also a misconceived impression that the Indian Navy was responsible for the complete response in the event of an aircraft disaster.
The main objective of the AEP is to reduce loss of life and limb and re-commence flight operations at the earliest. However, for a workable plan the following issues are relevant and considered essential:-
Formulation of Airport Energency Dean
Arrangement of emergency Mutual Aid Agreements. This agreement defines responsibilities and liabilities of each contributing party to disaster management. It also lays down procedures for coordinating responses within and between agencies. The same is and reviewed annually.
Resolution of major problem areas in command, communication and coordination.
Laying down jurisdiction in event of 'on' base and 'off' base accidents.
Sources of provision of manpower and equipment from available sources.
To formulate the new AEP for Dabolim airport, the above mentioned issues were forwarded as agenda points to all state agencies/AAI/Aircraft Operators which was soon followed by a meeting involving senior decision making representatives from each agency.
The various agencies involved were from the State administrative machinery, Director of Health Services, representatives from the law enforcement agency, AAI, aircraft operators, directors of major hospitals and Coast Guard. During the preliminary meetings it was also decided that a sub committee to better coordinate the medical aspects of the AEP be formed with the Director Health Services at the helm of this committee (Medical Core Group).
The first step taken was to clearly define the agency responsible for implementing the AEP in the event of an accident. The responsibility for handling a Civil aircraft accident on a Naval airport is with the State agencies and AAI with the Navy contributing under ‘Aid to Civil Power’. It was also understood that the Navy would immediately provide relief till the arrival of representatives of State Authorities/AAI.
The Command and Control, immediately after the accident, was thus defined as depicted in Figure 1.
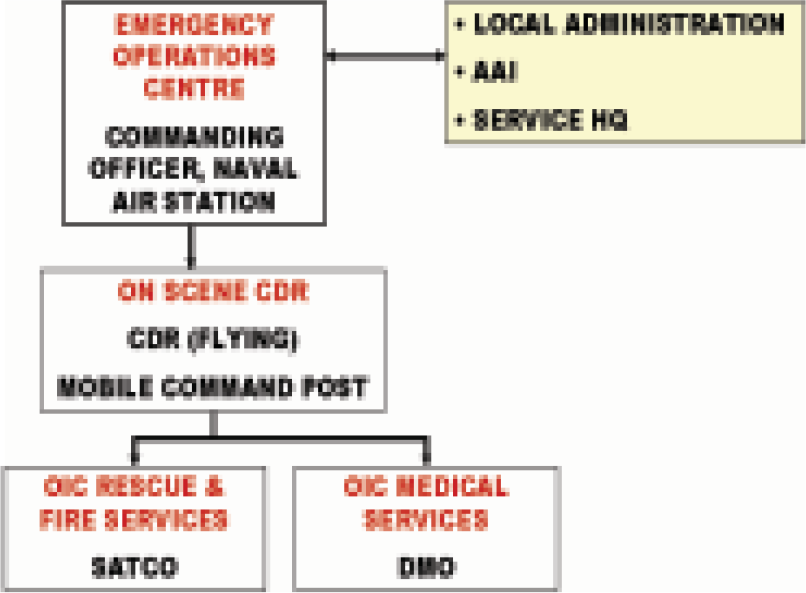
- Command and Control organisation at accident site immediately after a Civil Aircraft Accident
The AEP of the Naval Air station formulated was an extension of State Disaster Management plan. The various medical aspects of the AEP were defined at two levels namely:-
-
State and District Level
Organisation of Medical Services
Role of the Medical Core Group
Single Window Response System
-
Level of Naval Air Station
Assessment of magnitude of Medical Aid required.
Triage
Evacuation
Formulation of Medical Inventory – Manpower and Equipment.
Care of Ambulatory Survivors
Medical Plan: State and District Level
The medical services were organized under the leadership of Director Health Services (DHS). His functioning was through the Medical Core Group comprising of representatives from various medical Institutions. A hospital was identified which would function as the Medical Control Room at the time of emergency.
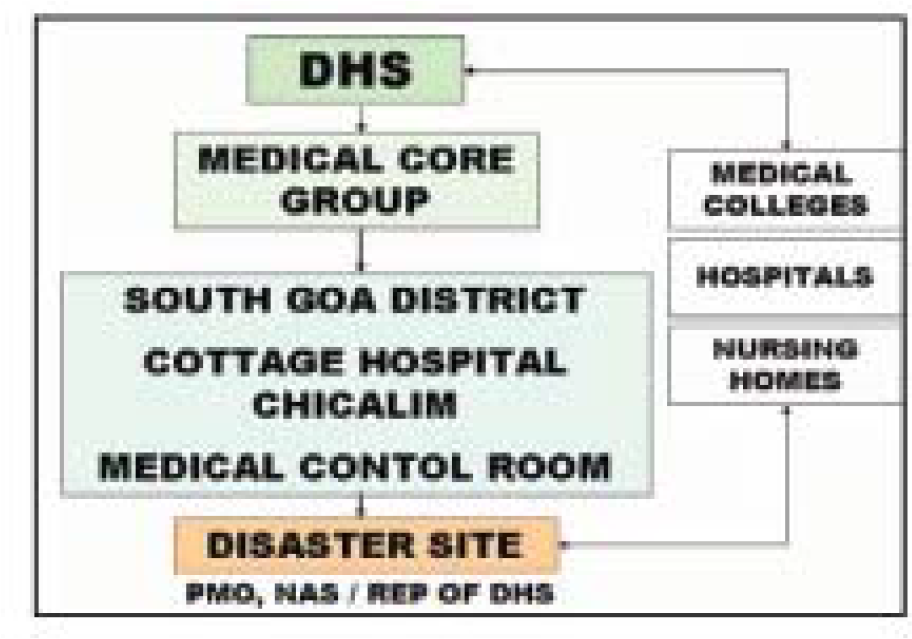
- Medical 'Command and Control' organisation implemented in the AEP of Dabolim Airport, Goa
The medical core group was required to play a key role in the medical response during an aircraft accident. It was the link between the medical services in the field and the state administration. Various tasks allocated to the medical core group were:-
Co-ordinate the dispatch of ambulances and response units.
Obtain feedback from field units, hospitals and medical professionals.
Inform hospitals/medical colleges/nursing homes at distant locations on possible need for beds & medical attention.
Coordinate/augment medical resources at site/hospitals.
Advise the District Commissioner on medical status and seek additional assistance.
Organise setting up of field treatment centers at schools/large halls near accident area for immediate medical attention. Mobilise manpower/supplies and support facilities for these centers.
Liaise with technical experts at hospitals and provide special medical advice to primary and secondary medical responders/field treatment centers.
The primary medical alarm, immediately after an aircraft accident, was based on the principal of a ‘Single Window Response System’ i.e. response action initiated by informing a single location. This was done through the already existing system installed at Goa i.e. GATES (Goa Accident and Trauma Emergency Service). A call on a single number would result in the local designated hospital assuming the role of Medical Control Room and the site at which all members of the Medical Core Group under Chairman, Director of Health Services, Goa would assemble at the earliest.
Medical Plan: Level of Naval Air Station
To define the magnitude of medical aid required at the critical aircraft accident most likely to pose the greatest problems for the medical organization was identified [1,8,9,10]. As per ICAO guidelines there are two approaches for defining the critical accident aircraft namely:-
Aircraft utilization factor: e.g. if the most frequent landing is by a) Boeing 737 on the airport with only an isolated landing by a larger aircraft the plan should be made to cater for the 737. The disaster plan for the Naval airport at Port Blair has been based on this factor.
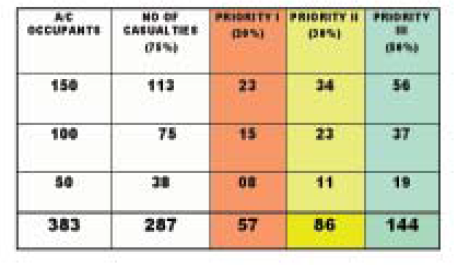
Capacity factor: However, if larger aircraft are landing on the airport frequently, then the plan should cater for the passenger capacity this aircraft can carry. The disaster management plan at Goa is based on this factor, with the airbus-330 with a total capacity of 383 personnel defined as the Critical Accident Aircraft. Thus in the worst case scenario, the number of casualties estimated is shown at table 1:-
Triage forms the basis of effective management of mass casualties. Using this system of sorting patients requires an in-depth knowledge of the Triage Card (Fug 3), and its correct usage. It also necessitated that all medical personnel whether from the military or civil be trained to carry out triage and have expertise of the level of Advance Trauma Life Support (ATLS) trained personnel.
A general outline of the evacuation plan is depicted in Fig 4 below. A pre-designated medical coordinator at the site of accident and pre-designated medical transport officer at the transport area were allocated specific responsibilities.
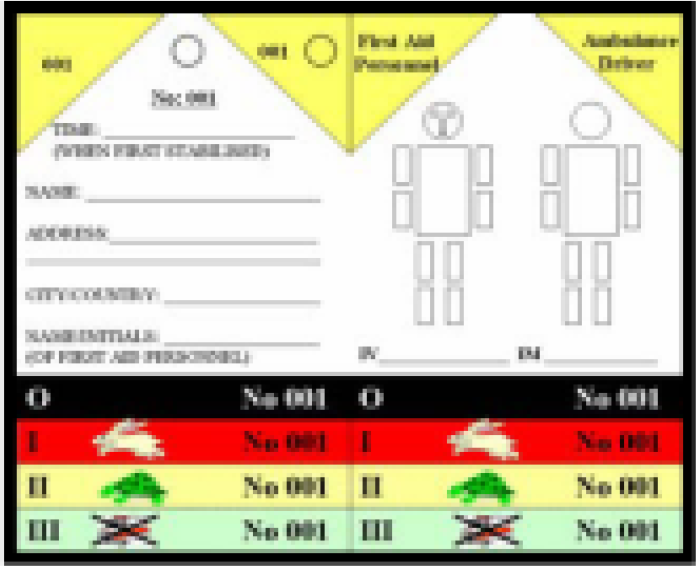
- Triage Card developed for Naval Air Station, INS Hansa
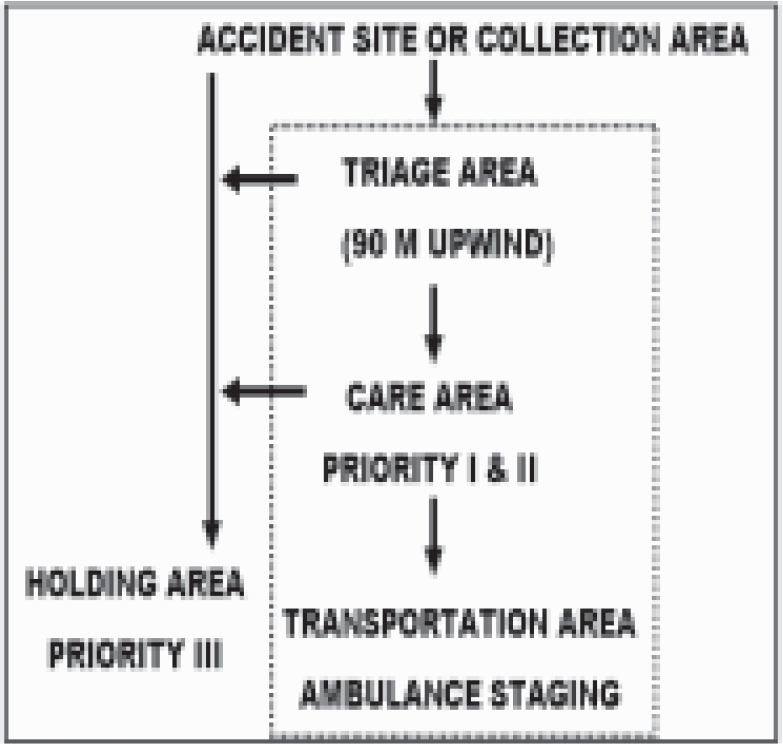
- Evacuation Plan
DHS tasked various medical organizations, AAI and Aircraft operators to provide a list of trained medical manpower and equipment that would be stocked and provided in the event of an accident. Medical equipment was intended to be stocked in the form of:-
Medical Bricks in the Naval Air Station.
Equipment that would be provided by various hospitals. A Medical Inventory indicating trained manpower, equipment and ambulances that would be provided by each hospital was to be provided by DHS.
AAI/Aircraft Operators were to ensure that the equipment recommended by ICAO be available on the airport.
A local pharmacy was to be identified by DHS which provide necessary medication immediately on demand.
Aircraft Operators were tasked to provide medical care and comfort to Priority III cases at the airport. Priority I and II cases were to be evacuated to designated hospitals
The success of any AEP depends on whether all personnel, military or civil, speak the same language. It was therefore important that the degree of training across all groups of paramedics be standardized, joint exercises undertaken and each understood the role they had to play. It was therefore proposed that DHS formulate a common training program (ATLS training).
Implementation of the AEP
The recommended frequency of exercise to test the AEP as laid down by ICAO [1] and other authors [11, 12] is drawn at Table 2.
| Full Scale Exercise | Once Every 02 Yrs |
|---|---|
| Partial Exercise | Once Every Yr |
| Table Top Exercise | Once Every 06 Months |
The table top exercise was found to be the easiest to implement which sensitized the participating agencies to the role they had to play. The aim of this exercise was to test integration and capability of emergency resources and reconfirm procedures, policy, telephone numbers, radio frequencies, changes in key personnel. It only required a meeting room, large scale map of the airport and senior members of each participating unit. A situation was injected and each participant had to describe the actions required to be undertaken.
Problem Areas
Several areas of concern after a table top/ partial exercise which changed are enumerated below:-
Inability of the State and Civil agencies to respond adequately in terms of manpower, equipment and ambulances during the conduct of exercises.
The delayed response time during a simulated emergency.
The level of training of paramedics to effectively contribute during an aircraft disaster was considered inadequate.
Conclusion
A single civil aircraft accident exposed the inadequacy of the existing AEP necessitating changes. This paper describes the various steps taken to affect changes in the existing AEP. This included sensitizing the State administration of its role in aircraft disaster management on a military airfield and military-civil interaction at the highest level of the state government. Dating the Medical organization at the state level, the role of the medical core group, assessment of magnitude of problem in the form of Critical Accident Aircraft, single window response system and formulating a medical inventory (manpower and equipment) and their sources were major areas of focus. Once formulated the plan was implemented and tested in the form of table top exercises and partial exercises. Areas of concern were mainly due to the delayed response of state/civil agencies and commitment of resources (manpower and equipment). Training remains a problem area which requires to be improved upon regularly.
As for the crashed Sahara aircraft, there were no passengers on board and the crew though shaken were unhurt. However, this accident revealed the lacunae in the existing plan. Though several issues have been resolved a lot still remains to be done to have an efficient AEP in place.
References
- Twenty years of medical support in aircraft disasters at Kennedy airport. Aerospace Med. 1973;44:560-6.
- [Google Scholar]
- Airport preparedness for mass disaster: a proposed schematic plan. Aviat Space Environ Med. 1986;57:77-81.
- [Google Scholar]
- Role of crisis intervention in an airport disaster plan. Aviat Space Environ Med. 1980;51:1260-2.
- [Google Scholar]
- Developing an emergency medical disaster plan for an airport. Aviat Space Environ Med. 1980;51:1258-9.
- [Google Scholar]
- Medical coordination in airport disasters. Aviat Space Environ Med. 1980;51:1256-8.
- [Google Scholar]
- Mass fatality aircraft disaster processing. Aviat Space Environ Med. 1989;60:A64-A73.
- [Google Scholar]
- Probability of casualties in an airport disaster. Aviat Space Environ Med. 1975;46:958-61.
- [Google Scholar]
- Mobilization of trauma teams for aircraft disasters. Aviat Space Environ Med. 1980;51:1262-6.
- [Google Scholar]




